{"title":"Ganglion Formation After Steroid Injection for Stenosing Flexor Tenosynovitis.","authors":"Kazuhiro Kohata, Yutaka Morizaki, Takafumi Miyake, Kosuke Uehara, Ryota Sugimura, Yasuhide Iwanaga, Sayaka Komine, Sakae Tanaka","doi":"10.2106/JBJS.OA.25.00152","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The exact mechanism underlying flexor tendon sheath ganglion (FTSG) formation remains unclear. We hypothesized that steroid injections into the A1 pulley are a cause of FTSG. Therefore, this study aimed to evaluate the risk of FTSG after steroid injections in patients with stenosing flexor tenosynovitis.</p><p><strong>Methods: </strong>This prospective cohort study enrolled patients diagnosed with stenosing flexor tenosynovitis between August 2019 and May 2024. A total of 128 fingers in 114 patients with no history of injections within the past 6 months consented to participate in the study. An initial ultrasound of the A1 pulley was performed, and patients with preexisting FTSG were excluded. Based on patient preference, the injection group received a steroid injection (5 mg of triamcinolone + 0.5 ml of 1% lidocaine) into the flexor tendon sheath, followed by a follow-up ultrasound at 3 months. The control group underwent ultrasonography at the same time points without injections.</p><p><strong>Results: </strong>Three-month follow-up ultrasound evaluations were conducted on 53 fingers (43 patients) in the injection group and 22 fingers (21 patients) in the control group. The incidence of FTSG was significantly higher in the injection group, with 20 of 53 fingers (37.7%) developing FTSG compared with 1 of 22 fingers (4.5%) in the control group. The risk difference was 0.33 (95% confidence interval: 0.18-0.49; p < 0.01). Symptom improvement was observed in 93% of the injection group compared with 45% of the control group (p < 0.01), indicating more significant symptom relief in the injection group.</p><p><strong>Conclusions: </strong>This study concluded that small punctures caused by steroid injections for stenosing flexor tenosynovitis can lead to FTSG; however, further studies are required to fully elucidate the clinical significance of ganglion formation.</p><p><strong>Level of evidence: </strong>Level II. See Instructions for Authors for a complete description of levels of evidence.</p>","PeriodicalId":36492,"journal":{"name":"JBJS Open Access","volume":"10 3","pages":""},"PeriodicalIF":3.8000,"publicationDate":"2025-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12366992/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBJS Open Access","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2106/JBJS.OA.25.00152","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The exact mechanism underlying flexor tendon sheath ganglion (FTSG) formation remains unclear. We hypothesized that steroid injections into the A1 pulley are a cause of FTSG. Therefore, this study aimed to evaluate the risk of FTSG after steroid injections in patients with stenosing flexor tenosynovitis.
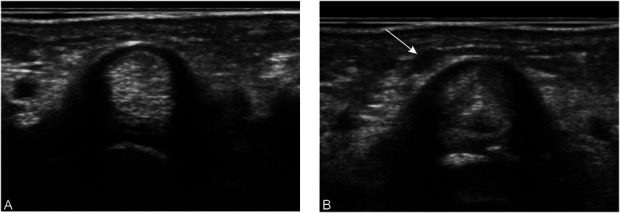
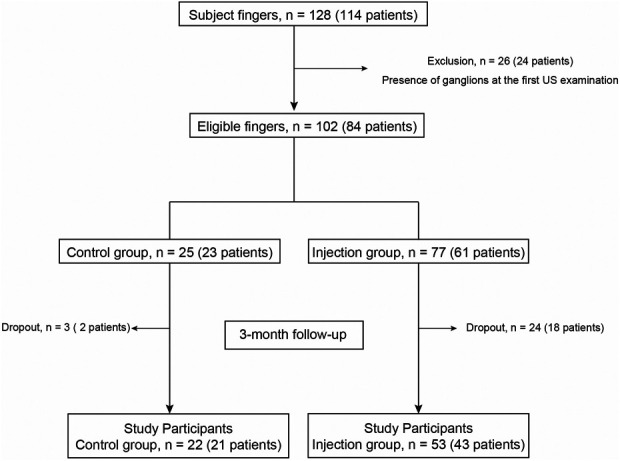
Methods: This prospective cohort study enrolled patients diagnosed with stenosing flexor tenosynovitis between August 2019 and May 2024. A total of 128 fingers in 114 patients with no history of injections within the past 6 months consented to participate in the study. An initial ultrasound of the A1 pulley was performed, and patients with preexisting FTSG were excluded. Based on patient preference, the injection group received a steroid injection (5 mg of triamcinolone + 0.5 ml of 1% lidocaine) into the flexor tendon sheath, followed by a follow-up ultrasound at 3 months. The control group underwent ultrasonography at the same time points without injections.
Results: Three-month follow-up ultrasound evaluations were conducted on 53 fingers (43 patients) in the injection group and 22 fingers (21 patients) in the control group. The incidence of FTSG was significantly higher in the injection group, with 20 of 53 fingers (37.7%) developing FTSG compared with 1 of 22 fingers (4.5%) in the control group. The risk difference was 0.33 (95% confidence interval: 0.18-0.49; p < 0.01). Symptom improvement was observed in 93% of the injection group compared with 45% of the control group (p < 0.01), indicating more significant symptom relief in the injection group.
Conclusions: This study concluded that small punctures caused by steroid injections for stenosing flexor tenosynovitis can lead to FTSG; however, further studies are required to fully elucidate the clinical significance of ganglion formation.
Level of evidence: Level II. See Instructions for Authors for a complete description of levels of evidence.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


