Young Rong Kim, Ha-Jin Chun, Jung Yeon Heo, Hakjun Hyun, Young Hwa Choi, Eun Jin Kim
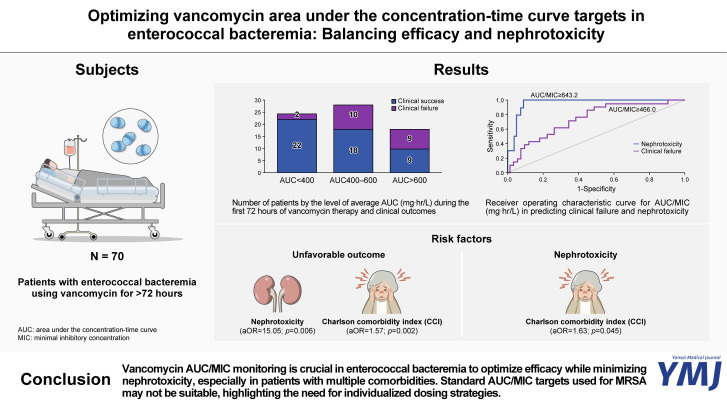
{"title":"Optimizing Vancomycin Area under the Concentration-Time Curve Targets in Enterococcal Bacteremia: Balancing Efficacy and Nephrotoxicity.","authors":"Young Rong Kim, Ha-Jin Chun, Jung Yeon Heo, Hakjun Hyun, Young Hwa Choi, Eun Jin Kim","doi":"10.3349/ymj.2024.0513","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Vancomycin is critical in treating enterococcal bacteremia; however, its optimal pharmacokinetic (PK)/pharmacodynamics (PD) targets remain unclear. This study evaluates the association between vancomycin PK/PD parameters and clinical outcomes in patients with enterococcal bacteremia.</p><p><strong>Materials and methods: </strong>This retrospective cohort study included 70 patients with enterococcal bacteremia treated with vancomycin at a university-affiliated teaching hospital. The primary and secondary outcomes were unfavorable clinical outcome (30-day mortality or persistent bacteremia) and nephrotoxicity, respectively. Vancomycin area under the concentration-time curve (AUC)/minimal inhibitory concentration (MIC) was calculated using Bayesian methods. Receiver operating curve (ROC) analysis determined AUC/MIC thresholds for predicting unfavorable clinical outcomes and nephrotoxicity. Logistic regression analysis identified risk factors for clinical outcomes.</p><p><strong>Results: </strong>Unfavorable outcome occurred in 21 patients (30.0%), and 10 (14.3%) experienced nephrotoxicity. The ROC-derived AUC₂₄/MIC cutoff for unfavorable outcome and nephrotoxicity were AUC₂₄/MIC ≥466.0 [AUC=0.740; 95% confidence interval (CI), 0.618-0.862] and ≥643.2 (AUC=0.963; 95% CI, 0.922-1.000), respectively. Clinical success was achieved in 44.9% (22/49) of patients with an AUC₂₄/MIC <400, whereas 47.6% (10/21) experienced unfavorable outcome despite having an AUC₂₄/MIC of 400-600. Nephrotoxicity [adjusted odds ratio (aOR)=15.05; 95% CI, 2.15-105.14; <i>p</i>=0.006] and Charlson Comorbidity Index (CCI) (aOR=1.57; 95% CI, 1.18-2.08; <i>p</i>=0.002) were independent risk factors for unfavorable outcome. High AUC₂₄/MIC and CCI were associated with nephrotoxicity (aOR=1.03; 95% CI, 1.01-1.04; <i>p</i>=0.005, and aOR=1.83; 95% CI, 1.01-3.35; <i>p</i>=0.045).</p><p><strong>Conclusion: </strong>Nephrotoxicity and multiple comorbidities were stronger risk factors for unfavorable outcomes than vancomycin AUC/MIC. These findings highlight the need for individualized strategies to optimize efficacy while minimizing toxicity. Further large-scale studies are warranted to refine the optimal AUC/MIC threshold.</p>","PeriodicalId":23765,"journal":{"name":"Yonsei Medical Journal","volume":"66 9","pages":"609-617"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12394755/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Yonsei Medical Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3349/ymj.2024.0513","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Vancomycin is critical in treating enterococcal bacteremia; however, its optimal pharmacokinetic (PK)/pharmacodynamics (PD) targets remain unclear. This study evaluates the association between vancomycin PK/PD parameters and clinical outcomes in patients with enterococcal bacteremia.
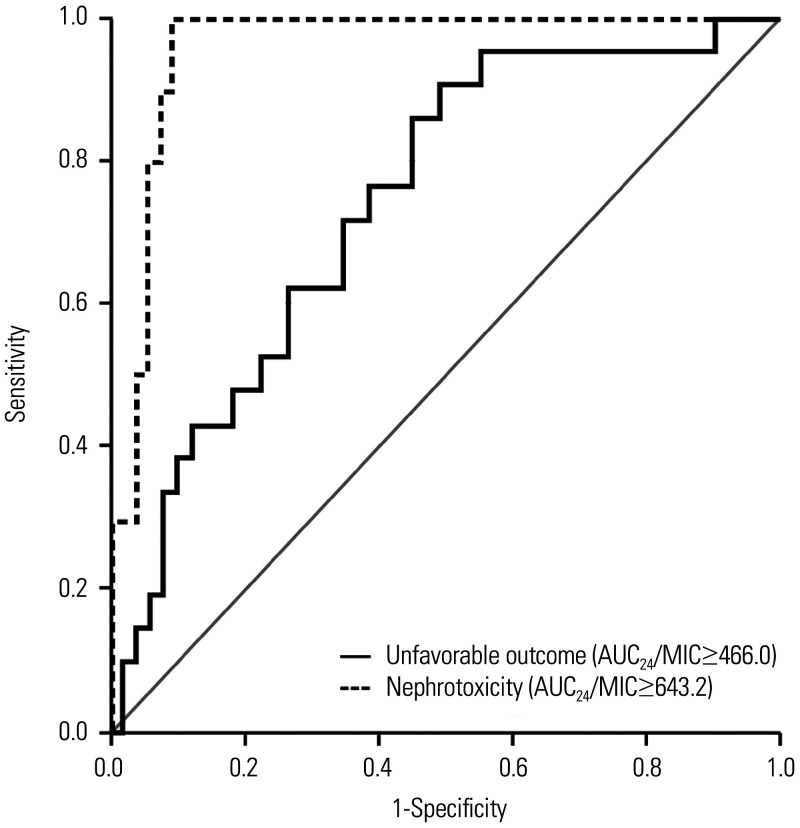
Materials and methods: This retrospective cohort study included 70 patients with enterococcal bacteremia treated with vancomycin at a university-affiliated teaching hospital. The primary and secondary outcomes were unfavorable clinical outcome (30-day mortality or persistent bacteremia) and nephrotoxicity, respectively. Vancomycin area under the concentration-time curve (AUC)/minimal inhibitory concentration (MIC) was calculated using Bayesian methods. Receiver operating curve (ROC) analysis determined AUC/MIC thresholds for predicting unfavorable clinical outcomes and nephrotoxicity. Logistic regression analysis identified risk factors for clinical outcomes.
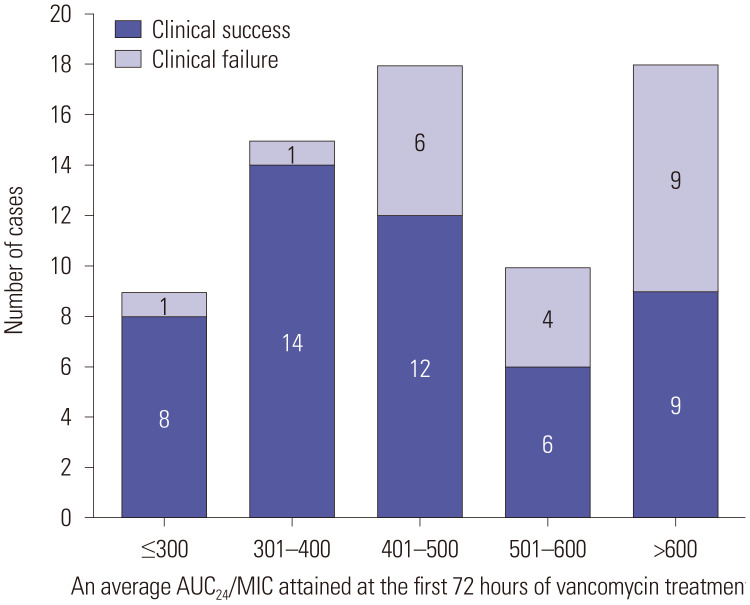
Results: Unfavorable outcome occurred in 21 patients (30.0%), and 10 (14.3%) experienced nephrotoxicity. The ROC-derived AUC₂₄/MIC cutoff for unfavorable outcome and nephrotoxicity were AUC₂₄/MIC ≥466.0 [AUC=0.740; 95% confidence interval (CI), 0.618-0.862] and ≥643.2 (AUC=0.963; 95% CI, 0.922-1.000), respectively. Clinical success was achieved in 44.9% (22/49) of patients with an AUC₂₄/MIC <400, whereas 47.6% (10/21) experienced unfavorable outcome despite having an AUC₂₄/MIC of 400-600. Nephrotoxicity [adjusted odds ratio (aOR)=15.05; 95% CI, 2.15-105.14; p=0.006] and Charlson Comorbidity Index (CCI) (aOR=1.57; 95% CI, 1.18-2.08; p=0.002) were independent risk factors for unfavorable outcome. High AUC₂₄/MIC and CCI were associated with nephrotoxicity (aOR=1.03; 95% CI, 1.01-1.04; p=0.005, and aOR=1.83; 95% CI, 1.01-3.35; p=0.045).
Conclusion: Nephrotoxicity and multiple comorbidities were stronger risk factors for unfavorable outcomes than vancomycin AUC/MIC. These findings highlight the need for individualized strategies to optimize efficacy while minimizing toxicity. Further large-scale studies are warranted to refine the optimal AUC/MIC threshold.
期刊介绍:
The goal of the Yonsei Medical Journal (YMJ) is to publish high quality manuscripts dedicated to clinical or basic research. Any authors affiliated with an accredited biomedical institution may submit manuscripts of original articles, review articles, case reports, brief communications, and letters to the Editor.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


