The effects of Dexmedetomidine on Recovery from Acute KIdney INjury (DRAIN): a single-center retrospective review using the Medical Information Mart for Intensive Care, fourth edition (MIMIC-IV).
{"title":"The effects of Dexmedetomidine on Recovery from Acute KIdney INjury (DRAIN): a single-center retrospective review using the Medical Information Mart for Intensive Care, fourth edition (MIMIC-IV).","authors":"James Harvey Jones, Susannah Fleming","doi":"10.1177/20420986251367509","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Dexmedetomidine may expedite recovery from acute kidney injury (AKI) in critically ill adults.</p><p><strong>Methods: </strong>This study utilizes data from the fourth edition of the Medical Information Mart for Intensive Care (MIMIC-IV). Adult patients admitted to Beth Israel Deaconess Medical Center in Boston, Massachusetts, between 2008 and 2019 with AKI and who have at least two serum creatinine values recorded in the MIMIC-IV database meet study inclusion criteria. The primary outcome measure is the time (days) from diagnosis of AKI to recovery. Secondary outcome measures are hospital and ICU length of stay (LOS) as well as in-hospital mortality.</p><p><strong>Results: </strong>A total of 1893 patients are included in this study. While 293 patients received dexmedetomidine, 1600 patients did not receive dexmedetomidine. Treatment with dexmedetomidine is associated with a 53.7% (95% CI: 46.8%-59.8%) decrease in the risk of recovery from AKI, on average, and this value is statistically significant (<i>p</i> < 0.001). Sensitivity analysis utilizing Cox regression of dexmedetomidine rate on time to AKI recovery demonstrated the opposite effect, however, with an adjusted HR of 1.42 (95% CI: 1.24-1.63, <i>p</i> value <0.001). Theories for this opposite effect are explored in the Discussion section of the manuscript. For patients who receive dexmedetomidine, hospital and ICU LOS, on average, increase by 18.98% and 32.56%, respectively (<i>p</i> value <0.001). Patients who receive dexmedetomidine have 0.6 times the odds of in-hospital mortality, on average, compared to patients who do not receive dexmedetomidine, which is statistically significant (<i>p</i> value 0.006).</p><p><strong>Conclusion: </strong>Dexmedetomidine may be associated with slower recovery from AKI in critically ill adults. The prolonged hospital and ICU LOS associated with dexmedetomidine may be related to reduced mortality, but these results require additional investigation. These exploratory results warrant further investigation to better understand the clinical implications of dexmedetomidine exposure in the setting of AKI.</p>","PeriodicalId":23012,"journal":{"name":"Therapeutic Advances in Drug Safety","volume":"16 ","pages":"20420986251367509"},"PeriodicalIF":3.4000,"publicationDate":"2025-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12368322/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20420986251367509","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Dexmedetomidine may expedite recovery from acute kidney injury (AKI) in critically ill adults.
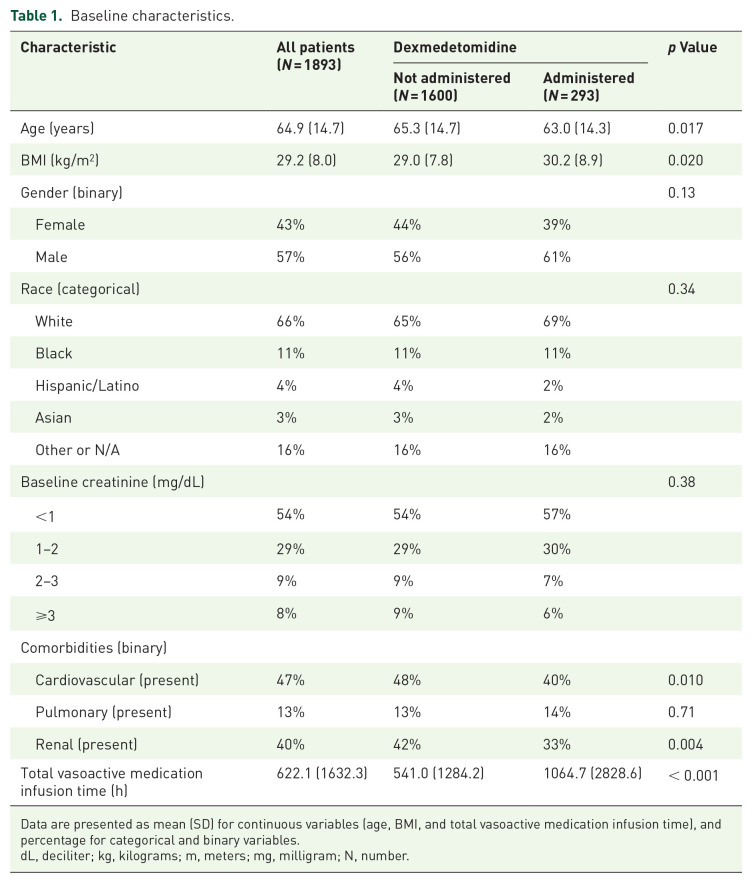
Methods: This study utilizes data from the fourth edition of the Medical Information Mart for Intensive Care (MIMIC-IV). Adult patients admitted to Beth Israel Deaconess Medical Center in Boston, Massachusetts, between 2008 and 2019 with AKI and who have at least two serum creatinine values recorded in the MIMIC-IV database meet study inclusion criteria. The primary outcome measure is the time (days) from diagnosis of AKI to recovery. Secondary outcome measures are hospital and ICU length of stay (LOS) as well as in-hospital mortality.
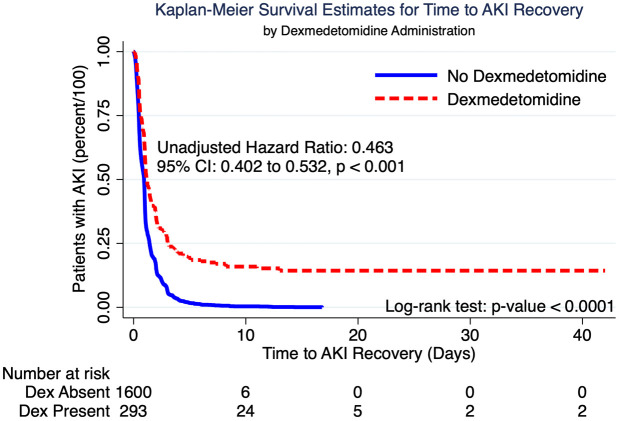
Results: A total of 1893 patients are included in this study. While 293 patients received dexmedetomidine, 1600 patients did not receive dexmedetomidine. Treatment with dexmedetomidine is associated with a 53.7% (95% CI: 46.8%-59.8%) decrease in the risk of recovery from AKI, on average, and this value is statistically significant (p < 0.001). Sensitivity analysis utilizing Cox regression of dexmedetomidine rate on time to AKI recovery demonstrated the opposite effect, however, with an adjusted HR of 1.42 (95% CI: 1.24-1.63, p value <0.001). Theories for this opposite effect are explored in the Discussion section of the manuscript. For patients who receive dexmedetomidine, hospital and ICU LOS, on average, increase by 18.98% and 32.56%, respectively (p value <0.001). Patients who receive dexmedetomidine have 0.6 times the odds of in-hospital mortality, on average, compared to patients who do not receive dexmedetomidine, which is statistically significant (p value 0.006).
Conclusion: Dexmedetomidine may be associated with slower recovery from AKI in critically ill adults. The prolonged hospital and ICU LOS associated with dexmedetomidine may be related to reduced mortality, but these results require additional investigation. These exploratory results warrant further investigation to better understand the clinical implications of dexmedetomidine exposure in the setting of AKI.
期刊介绍:
Therapeutic Advances in Drug Safety delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies pertaining to the safe use of drugs in patients.
The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in drug safety, providing a forum in print and online for publishing the highest quality articles in this area. The editors welcome articles of current interest on research across all areas of drug safety, including therapeutic drug monitoring, pharmacoepidemiology, adverse drug reactions, drug interactions, pharmacokinetics, pharmacovigilance, medication/prescribing errors, risk management, ethics and regulation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


