{"title":"Dose-dependent renoprotective effects of sacubitril/valsartan in heart failure: a retrospective study.","authors":"Takahiro Kato, Yusuke Nakano, Noriko Yasukawa, Masafumi Oonishi, Yukihiro Hamada","doi":"10.1080/0886022X.2025.2538830","DOIUrl":null,"url":null,"abstract":"<p><p>To evaluate the dose-dependent renoprotective effects of sacubitril/valsartan in heart failure patients. This retrospective observational study included patients with heart failure (Stage B or higher, B-type natriuretic peptide (BNP) >100 pg/mL or N-terminal proBNP >300 pg/mL) who initiated sacubitril/valsartan (SV) treatment. Patients were classified by final SV daily dose (50, 100, 200, or 400 mg) at 18 months. Factors associated with eGFR changes were identified using multiple regression analysis. A total of 157 patients (mean age 74.8-77.9 years, 64.3% male) were stratified by daily SV dosage groups (50 mg, <i>n</i> = 20; 100 mg, <i>n</i> = 46; 200 mg, <i>n</i> = 62; 400 mg, <i>n</i> = 29). Baseline characteristics were similar across groups for eGFR, heart failure stage, diabetes history, myocardial infarction, atrial fibrillation, proteinuria, and use of most heart failure medications. However, hypertension prevalence and systolic blood pressure differed significantly between groups (<i>p</i> < 0.05). One-way ANOVA revealed significant dose-dependent differences in eGFR changes among SV dosage groups (<i>p</i> < 0.05). In the final multiple linear regression model, SV dosage (<i>p</i> < 0.05) was a significant factor associated with eGFR changes, with proteinuria showing a trend toward significance. Sex and BNP levels ≥400 pg/dL were not significant. Sensitivity analysis converting SV dosage to a categorical variable confirmed these findings. Stratification by proteinuria status demonstrated dose-dependent relationships in both proteinuria-positive and proteinuria-negative subgroups, with more pronounced dose dependency in the proteinuria-positive group (<i>p</i> < 0.001). SV exhibits dose-dependent renoprotective effects in heart failure patients. Optimizing SV dosage may be beneficial for heart failure patients with concurrent kidney dysfunction, especially those with proteinuria.</p>","PeriodicalId":20839,"journal":{"name":"Renal Failure","volume":"47 1","pages":"2538830"},"PeriodicalIF":3.0000,"publicationDate":"2025-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12372510/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Renal Failure","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1080/0886022X.2025.2538830","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/21 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
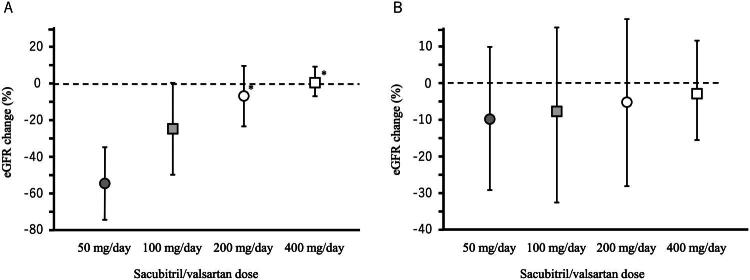
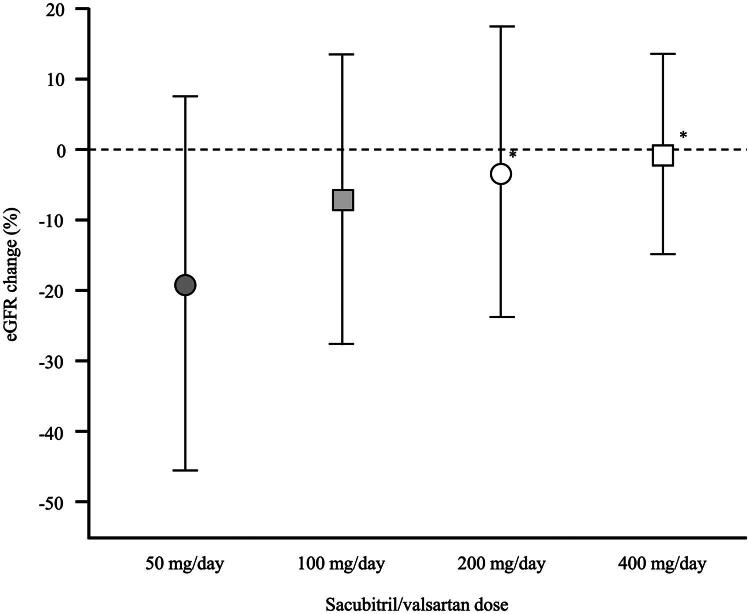
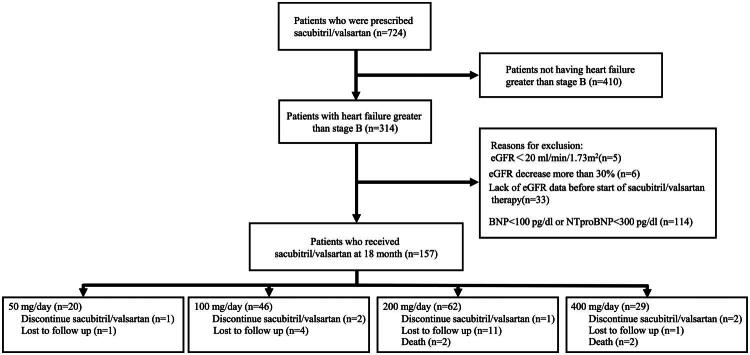
To evaluate the dose-dependent renoprotective effects of sacubitril/valsartan in heart failure patients. This retrospective observational study included patients with heart failure (Stage B or higher, B-type natriuretic peptide (BNP) >100 pg/mL or N-terminal proBNP >300 pg/mL) who initiated sacubitril/valsartan (SV) treatment. Patients were classified by final SV daily dose (50, 100, 200, or 400 mg) at 18 months. Factors associated with eGFR changes were identified using multiple regression analysis. A total of 157 patients (mean age 74.8-77.9 years, 64.3% male) were stratified by daily SV dosage groups (50 mg, n = 20; 100 mg, n = 46; 200 mg, n = 62; 400 mg, n = 29). Baseline characteristics were similar across groups for eGFR, heart failure stage, diabetes history, myocardial infarction, atrial fibrillation, proteinuria, and use of most heart failure medications. However, hypertension prevalence and systolic blood pressure differed significantly between groups (p < 0.05). One-way ANOVA revealed significant dose-dependent differences in eGFR changes among SV dosage groups (p < 0.05). In the final multiple linear regression model, SV dosage (p < 0.05) was a significant factor associated with eGFR changes, with proteinuria showing a trend toward significance. Sex and BNP levels ≥400 pg/dL were not significant. Sensitivity analysis converting SV dosage to a categorical variable confirmed these findings. Stratification by proteinuria status demonstrated dose-dependent relationships in both proteinuria-positive and proteinuria-negative subgroups, with more pronounced dose dependency in the proteinuria-positive group (p < 0.001). SV exhibits dose-dependent renoprotective effects in heart failure patients. Optimizing SV dosage may be beneficial for heart failure patients with concurrent kidney dysfunction, especially those with proteinuria.
评价苏比里尔/缬沙坦对心力衰竭患者的剂量依赖性肾保护作用。这项回顾性观察性研究纳入了接受苏比里尔/缬沙坦(SV)治疗的心力衰竭(B期或更高阶段,B型利钠肽(BNP) >100 pg/mL或n端proBNP >300 pg/mL)患者。患者在18个月时按最终SV日剂量(50,100,200或400mg)进行分类。使用多元回归分析确定与eGFR变化相关的因素。157例患者(平均年龄74.8 ~ 77.9岁,男性64.3%)按SV日剂量组(50 mg, n = 20; 100 mg, n = 46; 200 mg, n = 62; 400 mg, n = 29)进行分层。各组间eGFR、心力衰竭分期、糖尿病史、心肌梗死、心房颤动、蛋白尿和大多数心力衰竭药物使用的基线特征相似。然而,高血压患病率和收缩压组间差异显著(p p p p
期刊介绍:
Renal Failure primarily concentrates on acute renal injury and its consequence, but also addresses advances in the fields of chronic renal failure, hypertension, and renal transplantation. Bringing together both clinical and experimental aspects of renal failure, this publication presents timely, practical information on pathology and pathophysiology of acute renal failure; nephrotoxicity of drugs and other substances; prevention, treatment, and therapy of renal failure; renal failure in association with transplantation, hypertension, and diabetes mellitus.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


