Izak A R Yasrebi-de Kom, Kitty J Jager, Vianda S Stel, Nicholas C Chesnaye, Ameen Abu-Hanna, Nicolette F de Keizer, Dylan W de Lange, Dave A Dongelmans, Joanna E Klopotowska, Giovanni Cinà
{"title":"Vancomycin-Induced Acute Kidney Injury in Intensive Care Patients: A Target Trial Emulation Study Using Multicenter Routinely Collected Data.","authors":"Izak A R Yasrebi-de Kom, Kitty J Jager, Vianda S Stel, Nicholas C Chesnaye, Ameen Abu-Hanna, Nicolette F de Keizer, Dylan W de Lange, Dave A Dongelmans, Joanna E Klopotowska, Giovanni Cinà","doi":"10.1002/pds.70205","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The potential of vancomycin to cause acute kidney injury (AKI) in adult intensive care patients is subject to debate due to suboptimal designs of past studies. Therefore, we aimed to estimate the effect of initiating vancomycin versus one of several minimally nephrotoxic alternative antibiotics on the 14-day risk of AKI using the target trial emulation framework.</p><p><strong>Methods: </strong>A hypothetical trial was emulated using routinely collected data from 15 Dutch intensive care units (ICUs) spanning 2010-2019. We used an active comparator control group with the following alternative antibiotics: clindamycin, linezolid, teicoplanin, meropenem, cefazolin, and daptomycin. AKI was diagnosed according to the KDIGO serum creatinine (SCr) criteria. Cumulative incidence curves were estimated using the Aalen-Johansen method and adjusted for confounding and selection bias through inverse probability of treatment and censoring weighting. Given the time lag of 24-48 h between changes in renal function and SCr, we summarized the estimates by calculating the absolute risks and risk differences at both 2 and 14 days after initiation.</p><p><strong>Results: </strong>We included 1809 ICU admissions. After adjustment, vancomycin was associated with a higher risk of AKI at 14 days of follow-up compared to the alternative antibiotics (0.28 [95% confidence interval (CI) 0.21-0.34] vs. 0.17 [95% CI 0.14-0.20]; risk difference 0.11 [95% CI 0.04-0.19]), but not at 2 days of follow-up (0.10 [95% CI 0.06-0.12] vs. 0.10 [95% CI 0.08-0.11]; risk difference 0.00 [95% CI -0.03-0.03]).</p><p><strong>Conclusions: </strong>Our findings indicate that vancomycin causes a higher risk of AKI compared to the alternative antibiotics. We recommend clinicians to be compliant with vancomycin-induced AKI prevention strategies, such as therapeutic drug monitoring or the consideration of an alternative antibiotic if possible.</p>","PeriodicalId":19782,"journal":{"name":"Pharmacoepidemiology and Drug Safety","volume":"34 9","pages":"e70205"},"PeriodicalIF":2.4000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12394726/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pharmacoepidemiology and Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/pds.70205","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: The potential of vancomycin to cause acute kidney injury (AKI) in adult intensive care patients is subject to debate due to suboptimal designs of past studies. Therefore, we aimed to estimate the effect of initiating vancomycin versus one of several minimally nephrotoxic alternative antibiotics on the 14-day risk of AKI using the target trial emulation framework.
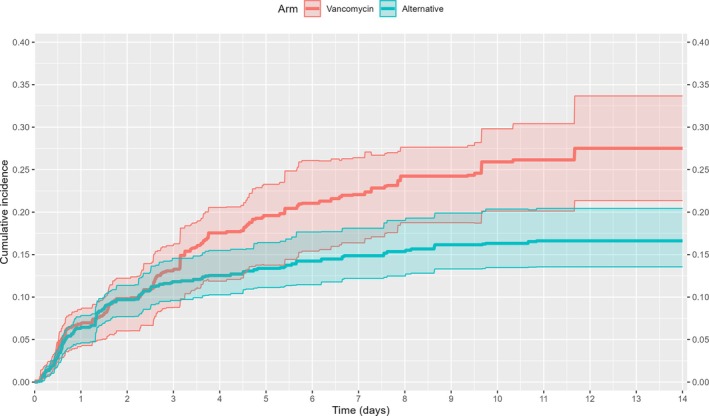
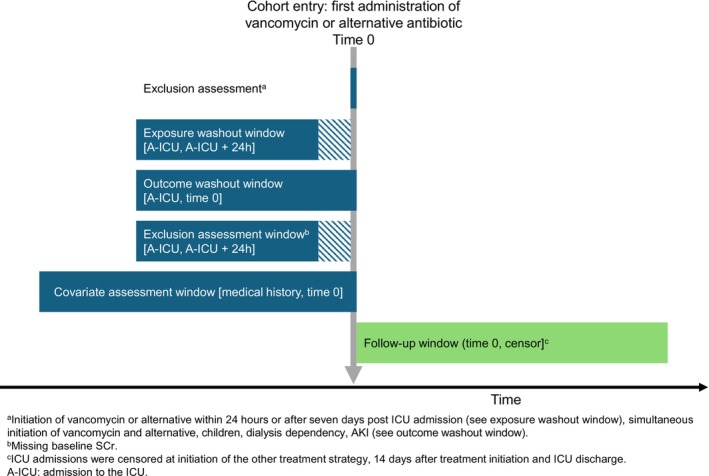
Methods: A hypothetical trial was emulated using routinely collected data from 15 Dutch intensive care units (ICUs) spanning 2010-2019. We used an active comparator control group with the following alternative antibiotics: clindamycin, linezolid, teicoplanin, meropenem, cefazolin, and daptomycin. AKI was diagnosed according to the KDIGO serum creatinine (SCr) criteria. Cumulative incidence curves were estimated using the Aalen-Johansen method and adjusted for confounding and selection bias through inverse probability of treatment and censoring weighting. Given the time lag of 24-48 h between changes in renal function and SCr, we summarized the estimates by calculating the absolute risks and risk differences at both 2 and 14 days after initiation.
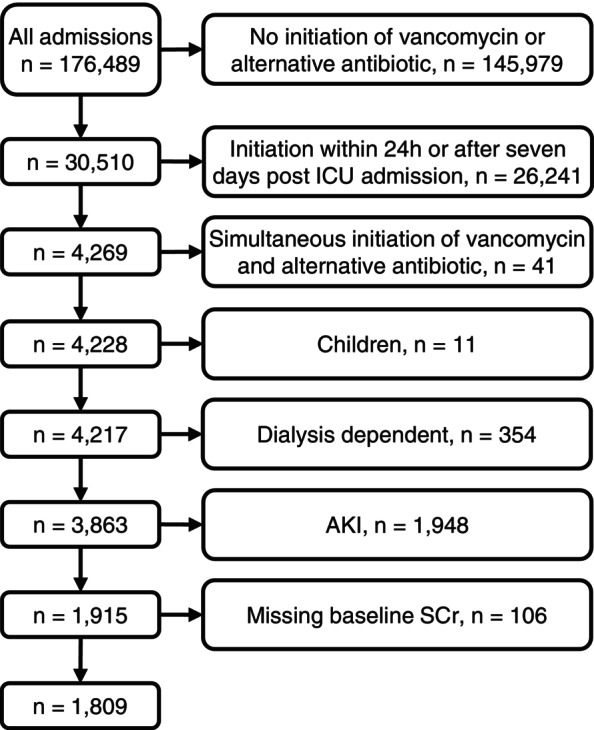
Results: We included 1809 ICU admissions. After adjustment, vancomycin was associated with a higher risk of AKI at 14 days of follow-up compared to the alternative antibiotics (0.28 [95% confidence interval (CI) 0.21-0.34] vs. 0.17 [95% CI 0.14-0.20]; risk difference 0.11 [95% CI 0.04-0.19]), but not at 2 days of follow-up (0.10 [95% CI 0.06-0.12] vs. 0.10 [95% CI 0.08-0.11]; risk difference 0.00 [95% CI -0.03-0.03]).
Conclusions: Our findings indicate that vancomycin causes a higher risk of AKI compared to the alternative antibiotics. We recommend clinicians to be compliant with vancomycin-induced AKI prevention strategies, such as therapeutic drug monitoring or the consideration of an alternative antibiotic if possible.
目的:万古霉素在成人重症监护患者中引起急性肾损伤(AKI)的可能性由于过去研究的次优设计而受到争议。因此,我们的目的是使用目标试验模拟框架来评估万古霉素与几种最低肾毒性替代抗生素中的一种对AKI 14天风险的影响。方法:使用2010-2019年期间从15个荷兰重症监护病房(icu)常规收集的数据模拟一项假设试验。我们使用了一个有活性的比较对照组,使用以下可选抗生素:克林霉素、利奈唑胺、替柯planin、美罗培南、头孢唑林和达托霉素。根据KDIGO血清肌酐(SCr)标准诊断AKI。使用aallen - johansen方法估计累积发生率曲线,并通过处理的逆概率和审查加权来调整混杂和选择偏差。考虑到肾功能变化与SCr之间的时间差为24-48小时,我们通过计算起始治疗后2天和14天的绝对风险和风险差异来总结估计。结果:我们纳入了1809例ICU入院患者。调整后,与其他抗生素相比,万古霉素与14天随访时AKI的风险较高(0.28[95%可信区间(CI) 0.21-0.34]对0.17 [95% CI 0.14-0.20];风险差0.11 [95% CI 0.04-0.19]),但随访2天无差异(0.10 [95% CI 0.06-0.12] vs. 0.10 [95% CI 0.08-0.11];风险差0.00 [95% CI -0.03-0.03])。结论:我们的研究结果表明,与其他抗生素相比,万古霉素引起AKI的风险更高。我们建议临床医生遵循万古霉素引起的AKI预防策略,如治疗药物监测或考虑替代抗生素。
期刊介绍:
The aim of Pharmacoepidemiology and Drug Safety is to provide an international forum for the communication and evaluation of data, methods and opinion in the discipline of pharmacoepidemiology. The Journal publishes peer-reviewed reports of original research, invited reviews and a variety of guest editorials and commentaries embracing scientific, medical, statistical, legal and economic aspects of pharmacoepidemiology and post-marketing surveillance of drug safety. Appropriate material in these categories may also be considered for publication as a Brief Report.
Particular areas of interest include:
design, analysis, results, and interpretation of studies looking at the benefit or safety of specific pharmaceuticals, biologics, or medical devices, including studies in pharmacovigilance, postmarketing surveillance, pharmacoeconomics, patient safety, molecular pharmacoepidemiology, or any other study within the broad field of pharmacoepidemiology;
comparative effectiveness research relating to pharmaceuticals, biologics, and medical devices. Comparative effectiveness research is the generation and synthesis of evidence that compares the benefits and harms of alternative methods to prevent, diagnose, treat, and monitor a clinical condition, as these methods are truly used in the real world;
methodologic contributions of relevance to pharmacoepidemiology, whether original contributions, reviews of existing methods, or tutorials for how to apply the methods of pharmacoepidemiology;
assessments of harm versus benefit in drug therapy;
patterns of drug utilization;
relationships between pharmacoepidemiology and the formulation and interpretation of regulatory guidelines;
evaluations of risk management plans and programmes relating to pharmaceuticals, biologics and medical devices.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


