Anticoagulation and antiplatelet strategies used in Sweden in patients with myocardial infarction and concomitant atrial fibrillation: nationwide cohort study.
Julia Aulin, Angelo Modica, Lars Lindhagen, Joakim Alfredsson, Claes Held, Stefan James, Gorav Batra
{"title":"Anticoagulation and antiplatelet strategies used in Sweden in patients with myocardial infarction and concomitant atrial fibrillation: nationwide cohort study.","authors":"Julia Aulin, Angelo Modica, Lars Lindhagen, Joakim Alfredsson, Claes Held, Stefan James, Gorav Batra","doi":"10.1136/openhrt-2025-003472","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Optimal antithrombotic therapy and its duration, whether triple therapy with dual antiplatelets plus oral anticoagulant (OAC), or dual antithrombotic therapy with an antiplatelet plus OAC, is uncertain for patients with myocardial infarction (MI) and atrial fibrillation (AF).</p><p><strong>Methods: </strong>Patients registered in SWEDEHEART (Swedish Web-system for enhancement and development of evidence-based care in heart disease evaluated according to recommended therapies) for their first MI between 2011 and 2021 with a history or new-onset AF were included (n=26 574). Linkage between SWEDEHEART and Swedish administrative health databases was performed, and pseudonymised data analysed.</p><p><strong>Results: </strong>Over time, OAC use at discharge after MI tripled from 27% in 2011 to 77% in 2021, with direct OACs (DOACs) largely replacing warfarin, predominantly in combination with a single antiplatelet. The strongest factors for initiating OAC therapy were the performance of coronary angiography (OR 1.53 (1.40-1.68)), and percutaneous coronary intervention (OR 1.49 (1.39-1.61)). However, the year of the MI was the most predictive variable associated with OAC initiation, with an OR of 9.31 (7.92-10.95) in 2021 compared with 2011. The clinical factors associated with lower likelihood of OAC initiation were dementia, liver disease, cancer and ST-elevation MI (STEMI) versus non-STEMI.</p><p><strong>Conclusions: </strong>Use of OAC has increased over the years in patients with MI and concurrent AF, primarily driven by the increased adoption of DOACs. Additionally, there has been a shift in antithrombotic combinations, with most patients in recent years receiving DOAC in combination with a single antiplatelet, reflecting the nationwide implementation of recent evidence and guidelines. However, significant variation in antithrombotic therapy strategies remains.</p>","PeriodicalId":19505,"journal":{"name":"Open Heart","volume":"12 2","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2025-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406944/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Heart","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/openhrt-2025-003472","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Optimal antithrombotic therapy and its duration, whether triple therapy with dual antiplatelets plus oral anticoagulant (OAC), or dual antithrombotic therapy with an antiplatelet plus OAC, is uncertain for patients with myocardial infarction (MI) and atrial fibrillation (AF).
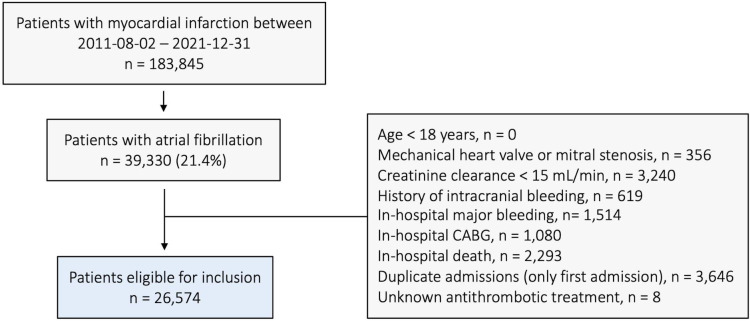
Methods: Patients registered in SWEDEHEART (Swedish Web-system for enhancement and development of evidence-based care in heart disease evaluated according to recommended therapies) for their first MI between 2011 and 2021 with a history or new-onset AF were included (n=26 574). Linkage between SWEDEHEART and Swedish administrative health databases was performed, and pseudonymised data analysed.
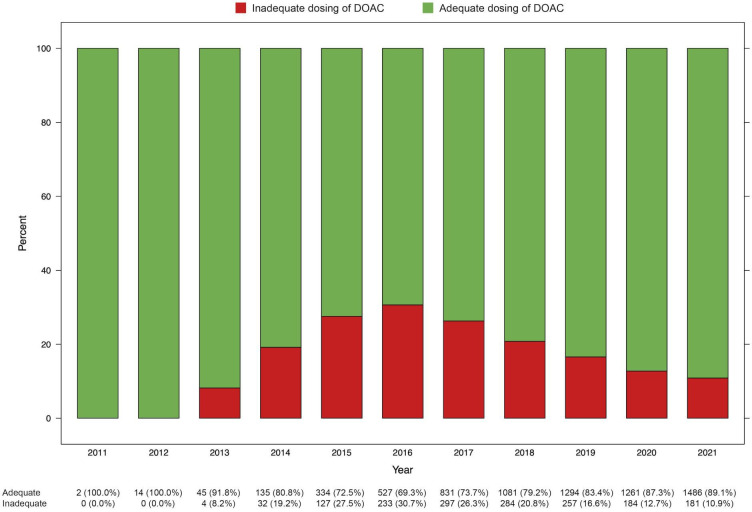
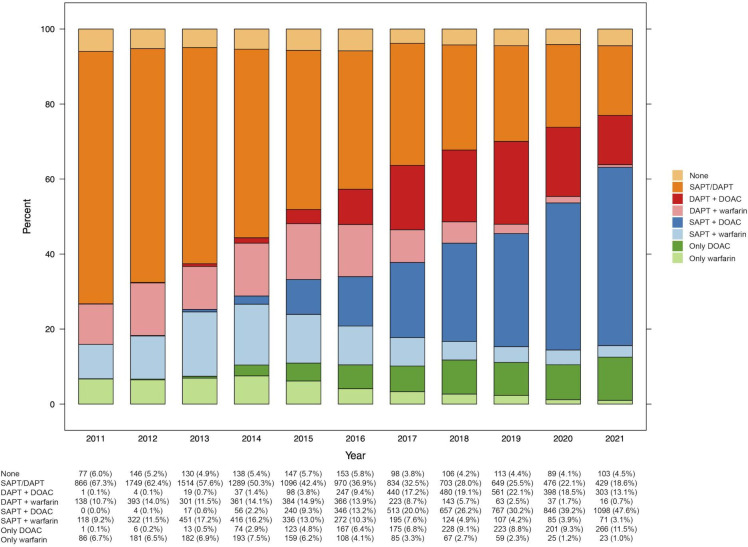
Results: Over time, OAC use at discharge after MI tripled from 27% in 2011 to 77% in 2021, with direct OACs (DOACs) largely replacing warfarin, predominantly in combination with a single antiplatelet. The strongest factors for initiating OAC therapy were the performance of coronary angiography (OR 1.53 (1.40-1.68)), and percutaneous coronary intervention (OR 1.49 (1.39-1.61)). However, the year of the MI was the most predictive variable associated with OAC initiation, with an OR of 9.31 (7.92-10.95) in 2021 compared with 2011. The clinical factors associated with lower likelihood of OAC initiation were dementia, liver disease, cancer and ST-elevation MI (STEMI) versus non-STEMI.
Conclusions: Use of OAC has increased over the years in patients with MI and concurrent AF, primarily driven by the increased adoption of DOACs. Additionally, there has been a shift in antithrombotic combinations, with most patients in recent years receiving DOAC in combination with a single antiplatelet, reflecting the nationwide implementation of recent evidence and guidelines. However, significant variation in antithrombotic therapy strategies remains.
期刊介绍:
Open Heart is an online-only, open access cardiology journal that aims to be “open” in many ways: open access (free access for all readers), open peer review (unblinded peer review) and open data (data sharing is encouraged). The goal is to ensure maximum transparency and maximum impact on research progress and patient care. The journal is dedicated to publishing high quality, peer reviewed medical research in all disciplines and therapeutic areas of cardiovascular medicine. Research is published across all study phases and designs, from study protocols to phase I trials to meta-analyses, including small or specialist studies. Opinionated discussions on controversial topics are welcomed. Open Heart aims to operate a fast submission and review process with continuous publication online, to ensure timely, up-to-date research is available worldwide. The journal adheres to a rigorous and transparent peer review process, and all articles go through a statistical assessment to ensure robustness of the analyses. Open Heart is an official journal of the British Cardiovascular Society.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


