Rahul R Karamchandani, Liang Wang, Hongmei Yang, Dale Strong, Jeremy B Rhoten, Jonathan D Clemente, Gary Defilipp, Elizabeth A Adelman, William R Stetler, Andrew W Asimos
{"title":"Validation of the Charlotte Large Artery Occlusion Endovascular Therapy Outcome Score in a Modern Cohort of Thrombectomy Patients.","authors":"Rahul R Karamchandani, Liang Wang, Hongmei Yang, Dale Strong, Jeremy B Rhoten, Jonathan D Clemente, Gary Defilipp, Elizabeth A Adelman, William R Stetler, Andrew W Asimos","doi":"10.3390/neurolint17080130","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/objectives: </strong>The Charlotte Large artery occlusion Endovascular therapy Outcome Score (CLEOS) predicts neurological outcomes after endovascular thrombectomy (EVT). Given recent expanded indications for EVT, we evaluated CLEOS in a modern cohort of thrombectomy patients.</p><p><strong>Methods: </strong>We retrospectively analyzed consecutive, anterior circulation EVT patients from January to December 2024 at multiple centers. The primary outcome was a 90-day modified Rankin Scale (mRS) score of 4-6. We compared primary outcome rates between the original CLEOS derivation cohort and the validation cohort. The area under the curve (AUC) was calculated for CLEOS and compared to other prognostic scales.</p><p><strong>Results: </strong>In the 347 included patients, the mean age was 67.6 (14.9) years, the median National Institutes of Health Stroke Scale (NIHSS) was 15 (10-20), and 137 (42.2%) had a 90-day mRS score of 4-6. A similar proportion of patients in the validation cohort and the derivation cohort achieved the primary outcome (39% each, <i>p</i> = 0.957). The AUC for CLEOS (0.7416, 95% confidence interval [CI] 0.688-0.795) was superior to that of the Pittsburgh Response to Endovascular therapy (AUC 0.681, 95% CI 0.624-0.738, <i>p</i> < 0.01) and Stroke Prognostication using Age and NIHSS (AUC 0.5982, 95% CI 0.556-0.640, <i>p</i> < 0.01), while a trend was observed compared to Houston Intra-Arterial Therapy-2 (AUC 0.6999, 95% CI 0.644-0.756, <i>p</i> = 0.0657) and Totaled Health Risk in Vascular Events (AUC 0.7046, 95% CI 0.560-0.759, <i>p</i> = 0.07). CLEOS ≥ 700 predicted the primary outcome in 16/19 (84.2%) patients.</p><p><strong>Conclusions: </strong>CLEOS performed well in our modern cohort of thrombectomy patients. Prognostic scales such as CLEOS may be useful in guiding conversations and setting expectations with family members pre- and post-thrombectomy.</p>","PeriodicalId":19130,"journal":{"name":"Neurology International","volume":"17 8","pages":""},"PeriodicalIF":3.0000,"publicationDate":"2025-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12388991/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology International","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/neurolint17080130","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background/objectives: The Charlotte Large artery occlusion Endovascular therapy Outcome Score (CLEOS) predicts neurological outcomes after endovascular thrombectomy (EVT). Given recent expanded indications for EVT, we evaluated CLEOS in a modern cohort of thrombectomy patients.
Methods: We retrospectively analyzed consecutive, anterior circulation EVT patients from January to December 2024 at multiple centers. The primary outcome was a 90-day modified Rankin Scale (mRS) score of 4-6. We compared primary outcome rates between the original CLEOS derivation cohort and the validation cohort. The area under the curve (AUC) was calculated for CLEOS and compared to other prognostic scales.
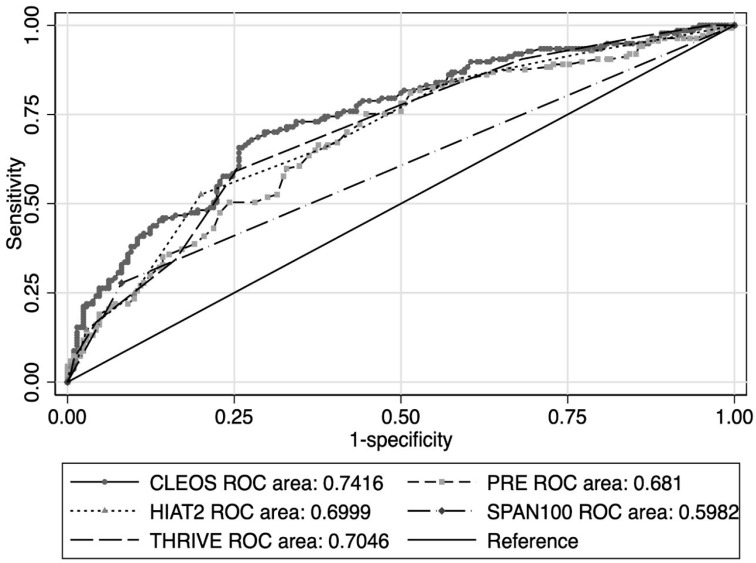
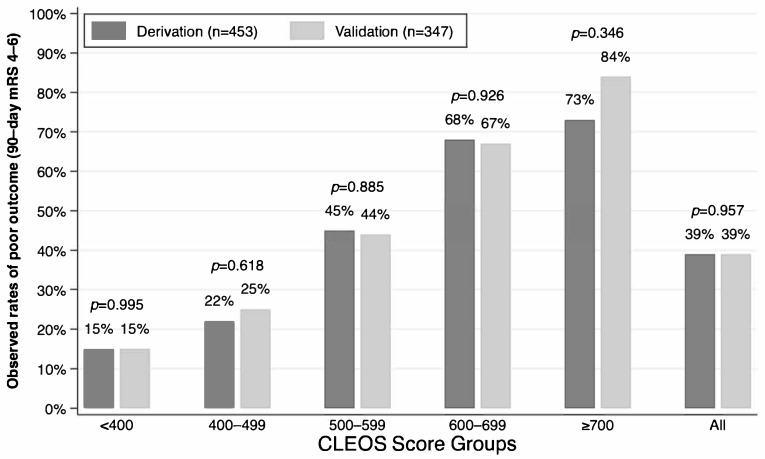
Results: In the 347 included patients, the mean age was 67.6 (14.9) years, the median National Institutes of Health Stroke Scale (NIHSS) was 15 (10-20), and 137 (42.2%) had a 90-day mRS score of 4-6. A similar proportion of patients in the validation cohort and the derivation cohort achieved the primary outcome (39% each, p = 0.957). The AUC for CLEOS (0.7416, 95% confidence interval [CI] 0.688-0.795) was superior to that of the Pittsburgh Response to Endovascular therapy (AUC 0.681, 95% CI 0.624-0.738, p < 0.01) and Stroke Prognostication using Age and NIHSS (AUC 0.5982, 95% CI 0.556-0.640, p < 0.01), while a trend was observed compared to Houston Intra-Arterial Therapy-2 (AUC 0.6999, 95% CI 0.644-0.756, p = 0.0657) and Totaled Health Risk in Vascular Events (AUC 0.7046, 95% CI 0.560-0.759, p = 0.07). CLEOS ≥ 700 predicted the primary outcome in 16/19 (84.2%) patients.
Conclusions: CLEOS performed well in our modern cohort of thrombectomy patients. Prognostic scales such as CLEOS may be useful in guiding conversations and setting expectations with family members pre- and post-thrombectomy.
背景/目的:夏洛特大动脉闭塞血管内治疗结局评分(CLEOS)预测血管内取栓(EVT)后的神经预后。鉴于最近EVT的适应症扩大,我们在现代血栓切除术患者队列中评估了CLEOS。方法:回顾性分析2024年1月至12月多个中心连续的前循环EVT患者。主要结果是90天的改良Rankin量表(mRS)评分为4-6分。我们比较了原始CLEOS衍生队列和验证队列的主要转归率。计算CLEOS的曲线下面积(AUC),并与其他预后量表进行比较。结果:纳入的347例患者平均年龄为67.6(14.9)岁,美国国立卫生研究院卒中量表(NIHSS)中位评分为15(10-20),137例(42.2%)患者90天mRS评分为4-6。验证队列和衍生队列中达到主要结局的患者比例相近(各39%,p = 0.957)。CLEOS的AUC(0.7416, 95%可信区间[CI] 0.668 -0.795)优于血管内治疗的匹兹堡反应(AUC 0.681, 95% CI 0.624-0.738, p < 0.01)和使用年龄和NIHSS进行卒中预后(AUC 0.5982, 95% CI 0.556-0.640, p < 0.01),而与休斯顿动脉内治疗-2 (AUC 0.6999, 95% CI 0.644-0.756, p = 0.0657)和血管事件的总健康风险(AUC 0.7046, 95% CI 0.560-0.759, p = 0.07)相比,有明显的趋势。CLEOS≥700预测16/19(84.2%)患者的主要结局。结论:CLEOS在我们的现代血栓切除术患者队列中表现良好。预后量表如CLEOS可用于指导血栓切除术前后与家庭成员的对话和设定期望。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


