Luís Felipe Leite, Luiz F Costa de Almeida, Samuel Menezes, Isabella Romagnoli, Daniel Dourado Striquer, Marcos Belotto
{"title":"Prophylactic abdominal drainage in pancreatic surgery: an updated systematic review and meta-analysis.","authors":"Luís Felipe Leite, Luiz F Costa de Almeida, Samuel Menezes, Isabella Romagnoli, Daniel Dourado Striquer, Marcos Belotto","doi":"10.1007/s00423-025-03763-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Prophylactic abdominal drainage has been widely used in pancreatic surgery to mitigate postoperative morbidity. Nonetheless, recent evidence suggests that a no-drain policy presents similar results to routine drainage. Therefore, we conducted an updated meta-analysis on this topic to provide up to date clinical recommendations.</p><p><strong>Methods: </strong>This systematic review and meta-analysis adhered to PRISMA guidelines and was registered in PROSPERO (CRD42024562683). A comprehensive search of Embase, MEDLINE, CENTRAL, and Web of Science was conducted up to June 2024. Included studies were RCTs comparing prophylactic drainage with no-drain strategies in pancreatic surgery. The ROB-2 tool and GRADE system were used for quality assessment.</p><p><strong>Results: </strong>Five RCTs with 1,337 patients (676 with drainage, 661 without) met inclusion criteria. Overall, no significant differences were observed in morbidity, major morbidity, intra-abdominal abscess, wound infection, hemorrhage, or reintervention rates between the two groups (moderate certainty evidence). Notably, the no-drain group had significantly lower 90-day mortality (RR 0.22; 95% CI 0.06-0.75; P < 0.05, moderate certainty evidence). In patients at low risk for POPF, prophylactic drainage was associated with a higher risk of developing POPF (RR 4.32; 95% CI 1.27-14.64; P < 0.05, low certainty evidence). No significant differences were found in patients at moderate or high risk for POPF.</p><p><strong>Discussion: </strong>Current evidence indicates that a no-drain policy is associated with comparable safety and efficiency outcomes to prophylactic drainage in pancreatic surgery, with similar mortality and morbidity profiles. In regards to CR-POPF incidence, a no drain policy is a non-inferior approach for PD, while in DP, prophylactic drainage is associated with a higher incidence of fistulas.</p>","PeriodicalId":17983,"journal":{"name":"Langenbeck's Archives of Surgery","volume":"410 1","pages":"255"},"PeriodicalIF":1.8000,"publicationDate":"2025-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12397327/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Langenbeck's Archives of Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00423-025-03763-z","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Prophylactic abdominal drainage has been widely used in pancreatic surgery to mitigate postoperative morbidity. Nonetheless, recent evidence suggests that a no-drain policy presents similar results to routine drainage. Therefore, we conducted an updated meta-analysis on this topic to provide up to date clinical recommendations.
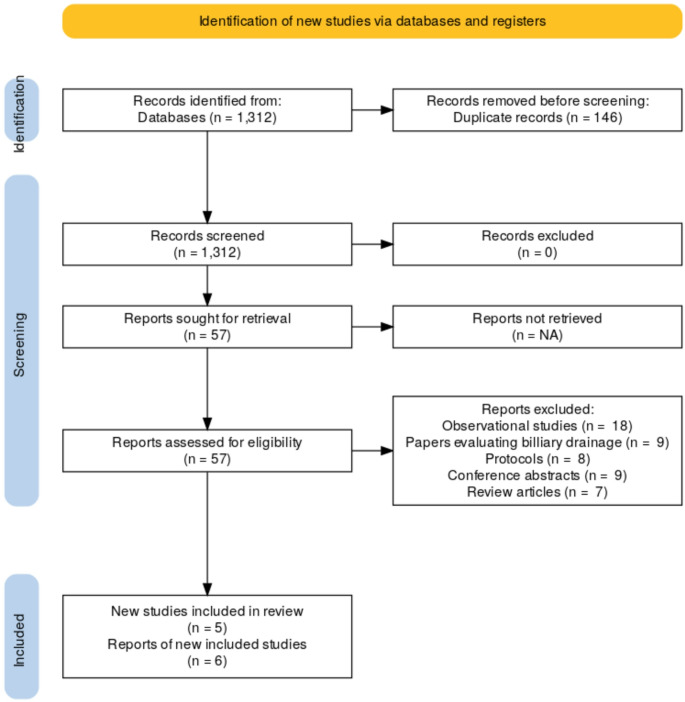
Methods: This systematic review and meta-analysis adhered to PRISMA guidelines and was registered in PROSPERO (CRD42024562683). A comprehensive search of Embase, MEDLINE, CENTRAL, and Web of Science was conducted up to June 2024. Included studies were RCTs comparing prophylactic drainage with no-drain strategies in pancreatic surgery. The ROB-2 tool and GRADE system were used for quality assessment.
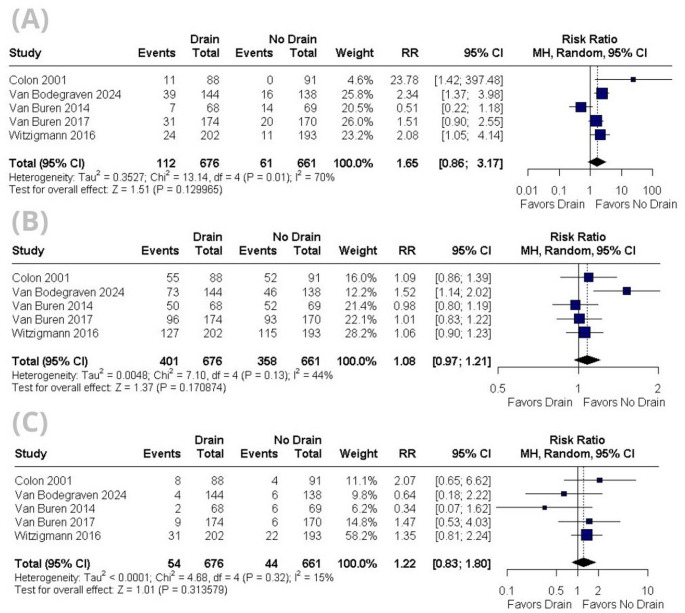
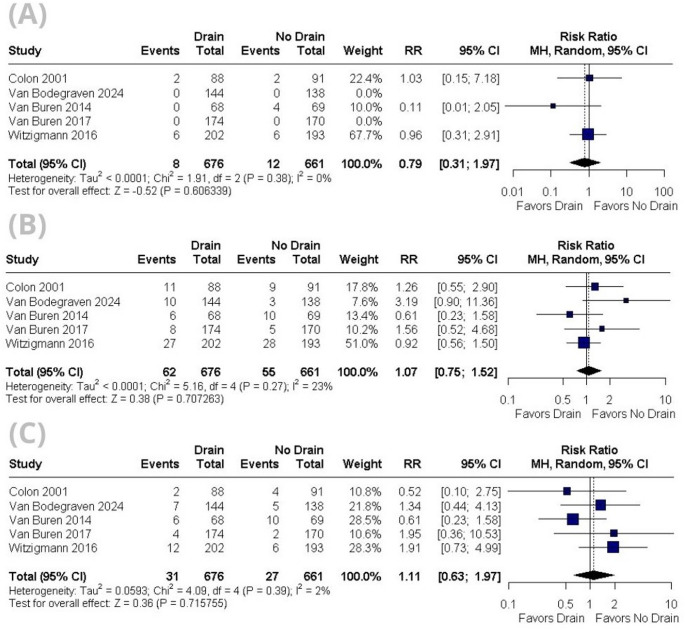
Results: Five RCTs with 1,337 patients (676 with drainage, 661 without) met inclusion criteria. Overall, no significant differences were observed in morbidity, major morbidity, intra-abdominal abscess, wound infection, hemorrhage, or reintervention rates between the two groups (moderate certainty evidence). Notably, the no-drain group had significantly lower 90-day mortality (RR 0.22; 95% CI 0.06-0.75; P < 0.05, moderate certainty evidence). In patients at low risk for POPF, prophylactic drainage was associated with a higher risk of developing POPF (RR 4.32; 95% CI 1.27-14.64; P < 0.05, low certainty evidence). No significant differences were found in patients at moderate or high risk for POPF.
Discussion: Current evidence indicates that a no-drain policy is associated with comparable safety and efficiency outcomes to prophylactic drainage in pancreatic surgery, with similar mortality and morbidity profiles. In regards to CR-POPF incidence, a no drain policy is a non-inferior approach for PD, while in DP, prophylactic drainage is associated with a higher incidence of fistulas.
背景:预防性腹腔引流术已广泛应用于胰腺手术,以减轻术后并发症。尽管如此,最近的证据表明,无排水政策的效果与常规排水相似。因此,我们对这一主题进行了更新的荟萃分析,以提供最新的临床建议。方法:该系统评价和荟萃分析遵循PRISMA指南,并在PROSPERO注册(CRD42024562683)。对Embase、MEDLINE、CENTRAL和Web of Science进行了全面的检索,截止到2024年6月。纳入的研究是比较胰腺手术预防性引流与无引流策略的随机对照试验。采用rob2工具和GRADE系统进行质量评价。结果:5项rct共1337例患者(676例引流,661例未引流)符合纳入标准。总体而言,两组在发病率、主要发病率、腹内脓肿、伤口感染、出血或再干预率方面无显著差异(中度确定性证据)。值得注意的是,无引流组的90天死亡率显著降低(RR 0.22; 95% CI 0.06-0.75; P)。讨论:目前的证据表明,在胰腺手术中,无引流政策与预防性引流具有相当的安全性和有效性,死亡率和发病率相似。关于CR-POPF的发生率,不引流政策是PD的非次等方法,而在DP中,预防性引流与较高的瘘管发生率相关。
期刊介绍:
Langenbeck''s Archives of Surgery aims to publish the best results in the field of clinical surgery and basic surgical research. The main focus is on providing the highest level of clinical research and clinically relevant basic research. The journal, published exclusively in English, will provide an international discussion forum for the controlled results of clinical surgery. The majority of published contributions will be original articles reporting on clinical data from general and visceral surgery, while endocrine surgery will also be covered. Papers on basic surgical principles from the fields of traumatology, vascular and thoracic surgery are also welcome. Evidence-based medicine is an important criterion for the acceptance of papers.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


