{"title":"Continuous Glucose Monitoring in Patients With Postbariatric Hypoglycemia: Effect on Hypoglycemia and Quality of Life.","authors":"Nicole Turk, Suruchi Ramanujan, Termeh Shamloo, Colleen Craig, Tracey McLaughlin","doi":"10.1210/jendso/bvaf106","DOIUrl":null,"url":null,"abstract":"<p><strong>Context: </strong>Postbariatric hypoglycemia (PBH), complicating up to one-third of bariatric surgeries, is characterized by repeated episodes of severe hypoglycemia and hypoglycemia unawareness that threaten patient safety and impair quality of life.</p><p><strong>Objective: </strong>We tested the hypothesis that use of a continuous glucose monitor (CGM) would reduce hypoglycemia and improve quality of life in patients with PBH.</p><p><strong>Design: </strong>In a crossover design, 14 patients with diagnosed PBH were assigned in random order to sequential treatment with unblinded CGM or blinded CGM/no alarms for 10 days each. Glucose and quality of life measures were compared between the 2 periods.</p><p><strong>Setting: </strong>Outpatient.</p><p><strong>Outcomes: </strong>Hypoglycemia measured by fingerstick blood glucose in response to symptoms or CGM alarm and CGM glucose values; quality of life measures included dietary liberalization and hypoglycemia-related worries/behaviors captured by the Hypoglycemia Fear Survey-II.</p><p><strong>Results: </strong>Baseline frequency of hypoglycemic events, disability, and hypoglycemia-related worries were high. Symptom-triggered hypoglycemic events confirmed by fingerstick glucose were reduced 6-fold (<i>P</i> = .008) and the glucose nadir measured by CGM was >8 mg/dL higher (<i>P</i> = .005) during unblinded use of CGM compared to the blinded comparison period. Hypoglycemia Fear Survey-II scores improved significantly in response to unblinded CGM use compared to the blinded control period (<i>P</i> = .026). The intake of carbohydrate-containing meals increased without increasing rate of postprandial hyper- or hypoglycemia.</p><p><strong>Conclusion: </strong>Use of unblinded CGM in patients with PBH reduces frequency and severity of hypoglycemia and improves quality of life by decreasing hypoglycemia-related worries and enabling a less restrictive diet. CGM should be considered a first-line treatment for patients with PBH.</p>","PeriodicalId":17334,"journal":{"name":"Journal of the Endocrine Society","volume":"9 9","pages":"bvaf106"},"PeriodicalIF":3.1000,"publicationDate":"2025-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12371835/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Endocrine Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jendso/bvaf106","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Context: Postbariatric hypoglycemia (PBH), complicating up to one-third of bariatric surgeries, is characterized by repeated episodes of severe hypoglycemia and hypoglycemia unawareness that threaten patient safety and impair quality of life.
Objective: We tested the hypothesis that use of a continuous glucose monitor (CGM) would reduce hypoglycemia and improve quality of life in patients with PBH.
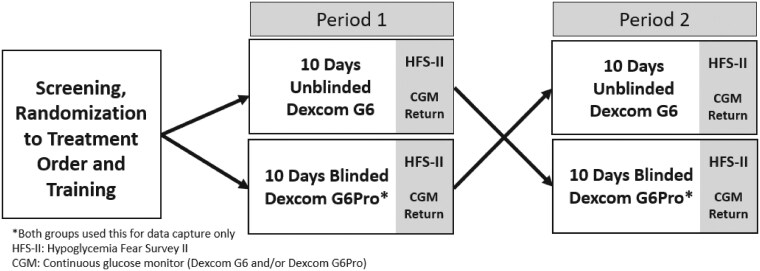
Design: In a crossover design, 14 patients with diagnosed PBH were assigned in random order to sequential treatment with unblinded CGM or blinded CGM/no alarms for 10 days each. Glucose and quality of life measures were compared between the 2 periods.
Setting: Outpatient.
Outcomes: Hypoglycemia measured by fingerstick blood glucose in response to symptoms or CGM alarm and CGM glucose values; quality of life measures included dietary liberalization and hypoglycemia-related worries/behaviors captured by the Hypoglycemia Fear Survey-II.
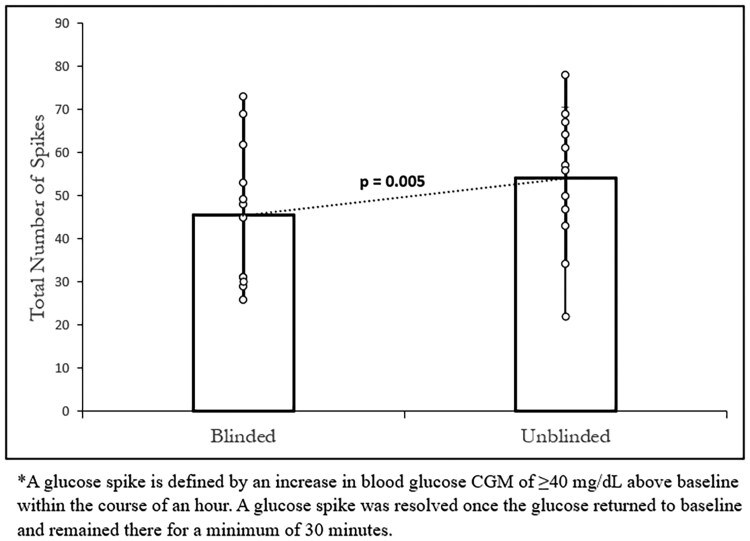
Results: Baseline frequency of hypoglycemic events, disability, and hypoglycemia-related worries were high. Symptom-triggered hypoglycemic events confirmed by fingerstick glucose were reduced 6-fold (P = .008) and the glucose nadir measured by CGM was >8 mg/dL higher (P = .005) during unblinded use of CGM compared to the blinded comparison period. Hypoglycemia Fear Survey-II scores improved significantly in response to unblinded CGM use compared to the blinded control period (P = .026). The intake of carbohydrate-containing meals increased without increasing rate of postprandial hyper- or hypoglycemia.
Conclusion: Use of unblinded CGM in patients with PBH reduces frequency and severity of hypoglycemia and improves quality of life by decreasing hypoglycemia-related worries and enabling a less restrictive diet. CGM should be considered a first-line treatment for patients with PBH.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


