{"title":"Pregnancy and Lactation Associated Bone Fragility.","authors":"Christopher S Kovacs","doi":"10.1210/jendso/bvaf126","DOIUrl":null,"url":null,"abstract":"<p><p>The skeleton is a storehouse of mineral that can be borrowed from in times of need, such as for reproduction. Skeletal resorption is normally modest during pregnancy but can be excessive when dietary calcium intake or absorption are insufficient for maternal and fetal needs. In contrast, substantial skeletal resorption is hormonally programmed to occur during lactation, with a loss of 5% to 10% of bone density from the spine over the first 6 months, independent of dietary calcium intake. The maternal skeleton is the main source of calcium in milk. Normally bone resorption during reproduction is without clinical consequences because the skeleton is restored to its prior mineral content and strength after weaning, such that parity and lactation are not risk factors for osteoporosis. However, bone strength is transiently reduced particularly during lactation, and can rarely lead to fragility fractures, especially if the skeleton was not normal before pregnancy. Women can present with fragility fractures during pregnancy but more often during lactation, sometimes with a frightening cascade of 5 to 10 vertebral compression fractures. This mini-review covers the epidemiology, pathophysiology, diagnostic approaches, and treatment considerations for this condition. Pharmacotherapy is often given in a desperate effort to do something, using agents that are not indicated in premenopausal women. The skeleton appears to recover, even in women who have fractured, such that it remains uncertain as to whether pharmacotherapy is necessary. Randomized trials are needed to determine when and in whom pharmacotherapy is needed, and which agent(s) might be preferable.</p>","PeriodicalId":17334,"journal":{"name":"Journal of the Endocrine Society","volume":"9 9","pages":"bvaf126"},"PeriodicalIF":3.1000,"publicationDate":"2025-07-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12362253/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Endocrine Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jendso/bvaf126","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
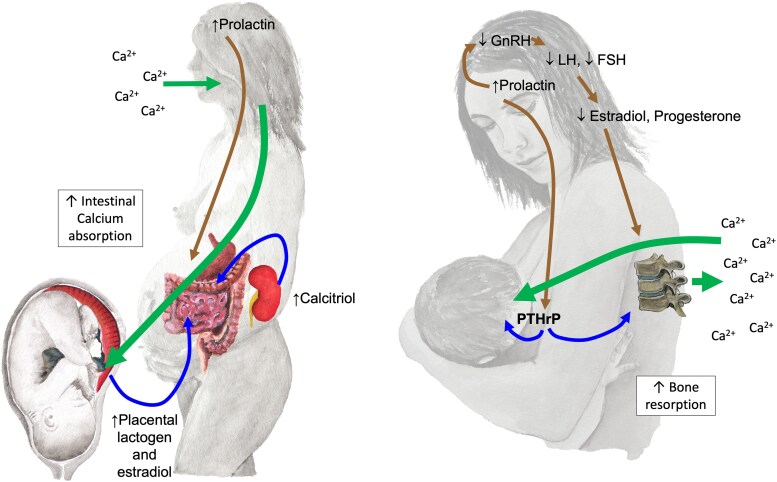
The skeleton is a storehouse of mineral that can be borrowed from in times of need, such as for reproduction. Skeletal resorption is normally modest during pregnancy but can be excessive when dietary calcium intake or absorption are insufficient for maternal and fetal needs. In contrast, substantial skeletal resorption is hormonally programmed to occur during lactation, with a loss of 5% to 10% of bone density from the spine over the first 6 months, independent of dietary calcium intake. The maternal skeleton is the main source of calcium in milk. Normally bone resorption during reproduction is without clinical consequences because the skeleton is restored to its prior mineral content and strength after weaning, such that parity and lactation are not risk factors for osteoporosis. However, bone strength is transiently reduced particularly during lactation, and can rarely lead to fragility fractures, especially if the skeleton was not normal before pregnancy. Women can present with fragility fractures during pregnancy but more often during lactation, sometimes with a frightening cascade of 5 to 10 vertebral compression fractures. This mini-review covers the epidemiology, pathophysiology, diagnostic approaches, and treatment considerations for this condition. Pharmacotherapy is often given in a desperate effort to do something, using agents that are not indicated in premenopausal women. The skeleton appears to recover, even in women who have fractured, such that it remains uncertain as to whether pharmacotherapy is necessary. Randomized trials are needed to determine when and in whom pharmacotherapy is needed, and which agent(s) might be preferable.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


