Costs of First-Line Treatment With FOLFIRINOX, Modified FOLFIRINOX, and Gemcitabine With Nab-Paclitaxel in Metastatic Pancreatic Ductal Adenocarcinoma.
Syvart Dennen, Marty Masek, Paul Cockrum, Elizabeth Nagelhout, Ravi Paluri
{"title":"Costs of First-Line Treatment With FOLFIRINOX, Modified FOLFIRINOX, and Gemcitabine With Nab-Paclitaxel in Metastatic Pancreatic Ductal Adenocarcinoma.","authors":"Syvart Dennen, Marty Masek, Paul Cockrum, Elizabeth Nagelhout, Ravi Paluri","doi":"10.36469/001c.142403","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Further research is needed to determine real-world costs of first-line (1L) treatment of metastatic pancreatic ductal adenocarcinoma (mPDAC) with FOLFIRINOX (FFX), modified FFX (mFFX), and gemcitabine with nab-paclitaxel (GnP).</p><p><strong>Objectives: </strong>To describe healthcare costs by treatment regimen, stratified by commercial and Medicare Advantage insurance.</p><p><strong>Methods: </strong>This retrospective cohort study of adult patients with mPDAC utilized Optum's de-identified Market Clarity Dataset. Demographics, clinical characteristics, and 1L unadjusted all-cause healthcare costs were examined. Total all-cause costs included costs from inpatient, outpatient, chemotherapy drug and administration, granulocyte colony-stimulating factor (G-CSF), radiation therapy, and other outpatient and pharmacy costs.</p><p><strong>Results: </strong>A total of 3115 patients met the criteria for inclusion and received 1L treatment with either FFX, mFFX, or GnP. Among those, 1703 had commercial insurance (FFX, 536; mFFX, 673; GnP, 494) and 1412 had Medicare Advantage (FFX, 201; mFFX, 317; GnP, 894). Total cost of care (mean [SD]) was similar between regimens for each insurance cohort (mean [SD] commercial: FFX, <math><mn>137</mn> <mrow><mo> </mo></mrow> <mn>813</mn> <mo>[</mo></math> 127 504]; mFFX, <math><mn>120</mn> <mrow><mo> </mo></mrow> <mn>109</mn> <mo>[</mo></math> 112 208]; GnP, <math><mn>133</mn> <mrow><mo> </mo></mrow> <mn>042</mn> <mo>[</mo></math> 154 248]; Medicare Advantage: FFX, <math><mn>110</mn> <mrow><mo> </mo></mrow> <mn>788</mn> <mo>[</mo></math> 98 492]; mFFX, <math><mn>98</mn> <mrow><mo> </mo></mrow> <mn>667</mn> <mo>[</mo></math> 83 437]; GnP, <math><mn>110</mn> <mrow><mo> </mo></mrow> <mn>211</mn> <mo>[</mo></math> 100 150]). For both insurance cohorts, chemotherapy drug costs were highest for GnP (mean [SD] commercial: FFX, <math><mn>10</mn> <mrow><mo> </mo></mrow> <mn>916</mn> <mo>[</mo></math> 21 647]; mFFX, <math><mn>7653</mn> <mo>[</mo></math> 10 054]; GnP, <math><mn>60</mn> <mrow><mo> </mo></mrow> <mn>466</mn> <mo>[</mo></math> 112 589]; Medicare Advantage: FFX, <math><mn>8028</mn> <mo>[</mo></math> 11 044]; mFFX, <math><mn>6016</mn> <mo>[</mo></math> 7688]; GnP, <math><mn>49</mn> <mrow><mo> </mo></mrow> <mn>263</mn> <mo>[</mo></math> 49 373]), while chemotherapy administration costs were higher for FFX and mFFX (commercial: FFX, <math><mn>25</mn> <mrow><mo> </mo></mrow> <mn>458</mn> <mo>[</mo></math> 33 350]; mFFX, <math><mn>22</mn> <mrow><mo> </mo></mrow> <mn>795</mn> <mo>[</mo></math> 24 309]; GnP <math><mn>12</mn> <mrow><mo> </mo></mrow> <mn>206</mn> <mo>[</mo></math> 15 766]; Medicare Advantage: FFX, <math><mn>25</mn> <mrow><mo> </mo></mrow> <mn>512</mn> <mo>[</mo></math> 36 352]; mFFX, <math><mn>21</mn> <mrow><mo> </mo></mrow> <mn>524</mn> <mo>[</mo></math> 22 317]; GnP <math><mn>11</mn> <mrow><mo> </mo></mrow> <mn>103</mn> <mo>[</mo></math> 13 089]). G-CSF costs were also higher for FFX and mFFX (commercial: FFX, <math><mn>38</mn> <mrow><mo> </mo></mrow> <mn>074</mn> <mo>[</mo></math> 56 593], mFFX, <math><mn>27</mn> <mrow><mo> </mo></mrow> <mn>823</mn> <mo>[</mo></math> 41 166]; GnP, <math><mn>4029</mn> <mo>[</mo></math> 14 181]; Medicare Advantage: FFX, <math><mn>30</mn> <mrow><mo> </mo></mrow> <mn>535</mn> <mo>[</mo></math> 56 630]; mFFX, <math><mn>24</mn> <mrow><mo> </mo></mrow> <mn>596</mn> <mo>[</mo></math> 39 286]; GnP, <math><mn>2412</mn> <mo>[</mo></math> 9115]).</p><p><strong>Discussion: </strong>Total costs of 1L FFX, mFFX, and GnP were similar within a commercially insured and Medicare Advantage cohort. FFX and mFFX costs were largely driven by chemotherapy administration and G-CSF costs, while GnP costs were driven by chemotherapy drug costs.</p><p><strong>Conclusions: </strong>To fully assess the economic impact of mPDAC in 1L treatment, it is essential to consider both the total cost and the individual cost components, such as chemotherapy drugs, administration, and supportive care costs.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"12 2","pages":"75-84"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12375408/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.142403","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Further research is needed to determine real-world costs of first-line (1L) treatment of metastatic pancreatic ductal adenocarcinoma (mPDAC) with FOLFIRINOX (FFX), modified FFX (mFFX), and gemcitabine with nab-paclitaxel (GnP).
Objectives: To describe healthcare costs by treatment regimen, stratified by commercial and Medicare Advantage insurance.
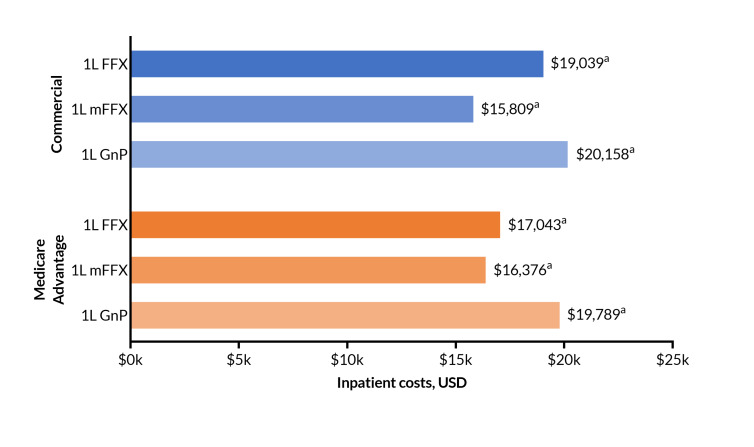
Methods: This retrospective cohort study of adult patients with mPDAC utilized Optum's de-identified Market Clarity Dataset. Demographics, clinical characteristics, and 1L unadjusted all-cause healthcare costs were examined. Total all-cause costs included costs from inpatient, outpatient, chemotherapy drug and administration, granulocyte colony-stimulating factor (G-CSF), radiation therapy, and other outpatient and pharmacy costs.
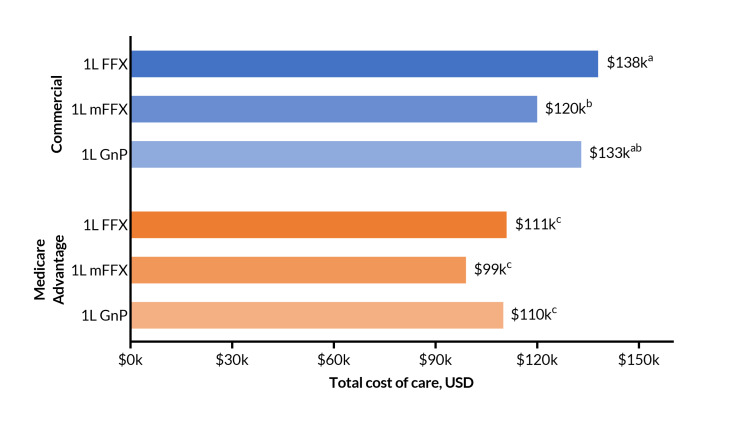
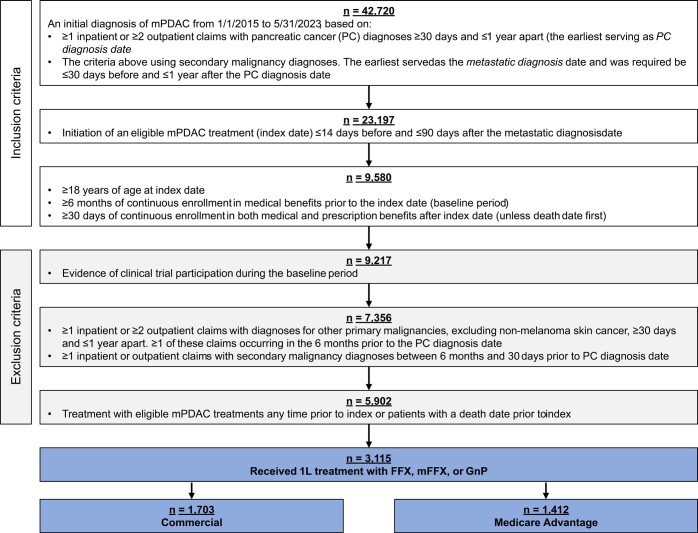
Results: A total of 3115 patients met the criteria for inclusion and received 1L treatment with either FFX, mFFX, or GnP. Among those, 1703 had commercial insurance (FFX, 536; mFFX, 673; GnP, 494) and 1412 had Medicare Advantage (FFX, 201; mFFX, 317; GnP, 894). Total cost of care (mean [SD]) was similar between regimens for each insurance cohort (mean [SD] commercial: FFX, 127 504]; mFFX, 112 208]; GnP, 154 248]; Medicare Advantage: FFX, 98 492]; mFFX, 83 437]; GnP, 100 150]). For both insurance cohorts, chemotherapy drug costs were highest for GnP (mean [SD] commercial: FFX, 21 647]; mFFX, 10 054]; GnP, 112 589]; Medicare Advantage: FFX, 11 044]; mFFX, 7688]; GnP, 49 373]), while chemotherapy administration costs were higher for FFX and mFFX (commercial: FFX, 33 350]; mFFX, 24 309]; GnP 15 766]; Medicare Advantage: FFX, 36 352]; mFFX, 22 317]; GnP 13 089]). G-CSF costs were also higher for FFX and mFFX (commercial: FFX, 56 593], mFFX, 41 166]; GnP, 14 181]; Medicare Advantage: FFX, 56 630]; mFFX, 39 286]; GnP, 9115]).
Discussion: Total costs of 1L FFX, mFFX, and GnP were similar within a commercially insured and Medicare Advantage cohort. FFX and mFFX costs were largely driven by chemotherapy administration and G-CSF costs, while GnP costs were driven by chemotherapy drug costs.
Conclusions: To fully assess the economic impact of mPDAC in 1L treatment, it is essential to consider both the total cost and the individual cost components, such as chemotherapy drugs, administration, and supportive care costs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


