Triple Therapy with Interventional Treatment, Donafenib, and Anti-PD-1 Antibodies in Unresectable Hepatocellular Carcinoma: A Retrospective Real-World Study in China.
Qiuwen Ye, Zhengrui Song, Tingdong Yu, Yong Li, Liang Ai, Guangjun Yang, Kun Su, Dong Chen, Wentao Zhao, Rong Ding, Yong Zha, Gang Li
{"title":"Triple Therapy with Interventional Treatment, Donafenib, and Anti-PD-1 Antibodies in Unresectable Hepatocellular Carcinoma: A Retrospective Real-World Study in China.","authors":"Qiuwen Ye, Zhengrui Song, Tingdong Yu, Yong Li, Liang Ai, Guangjun Yang, Kun Su, Dong Chen, Wentao Zhao, Rong Ding, Yong Zha, Gang Li","doi":"10.2147/JHC.S532120","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Unresectable hepatocellular carcinoma (uHCC) remains a major clinical challenge with limited effective therapeutic options. Triple therapy combining interventional treatments, donafenib, and anti-PD-1 monoclonal antibodies has shown promise in recent studies, but real-world data remain limited.</p><p><strong>Objective: </strong>To evaluate the real-world efficacy and safety of triple therapy with interventional treatment, donafenib, and anti-PD-1 monoclonal antibodies in patients with uHCC.</p><p><strong>Methods: </strong>This retrospective study included 89 patients with uHCC who received donafenib, anti-PD-1 monoclonal antibodies (tislelizumab or sintilimab), and interventional therapies (TACE and/or HAIC) between March 2022 and December 2023. Outcomes included objective response rate (ORR), progression-free survival (PFS), overall survival (OS), and safety. Efficacy was assessed using modified RECIST (mRECIST) criteria; prognostic factors were analyzed using Cox regression models.</p><p><strong>Results: </strong>Among 89 patients, the ORR was 75.3% and the disease control rate was 100%. The median PFS was 18.5 months (95% CI: 15.0-NA); median OS was not reached after a median follow-up of 13.7 months. PFS rates at 6, 12, and 18 months were 87.6%, 72.4%, and 52.7%, and OS rates were 93.3%, 81.6%, and 72.4%, respectively. Conversion surgery was achieved in 15.7% of patients. Subgroup analysis indicated that ECOG PS 1, extrahepatic metastases, and high baseline AFP were associated with worse survival outcomes, while interventional modality did not significantly affect prognosis. Multivariate analysis confirmed ECOG PS 1 and extrahepatic metastases as independent predictors of shorter PFS, and ECOG PS 1 and elevated AFP as independent predictors of worse OS. Grade ≥3 treatment-related adverse events occurred in 30.3% of patients; no treatment-related deaths were reported.</p><p><strong>Conclusion: </strong>The combination of interventional therapies, donafenib, and anti-PD-1 monoclonal antibodies demonstrated promising efficacy and manageable safety in uHCC, warranting further validation in prospective trials.</p>","PeriodicalId":15906,"journal":{"name":"Journal of Hepatocellular Carcinoma","volume":"12 ","pages":"1905-1919"},"PeriodicalIF":3.4000,"publicationDate":"2025-08-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12393086/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepatocellular Carcinoma","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/JHC.S532120","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Unresectable hepatocellular carcinoma (uHCC) remains a major clinical challenge with limited effective therapeutic options. Triple therapy combining interventional treatments, donafenib, and anti-PD-1 monoclonal antibodies has shown promise in recent studies, but real-world data remain limited.
Objective: To evaluate the real-world efficacy and safety of triple therapy with interventional treatment, donafenib, and anti-PD-1 monoclonal antibodies in patients with uHCC.
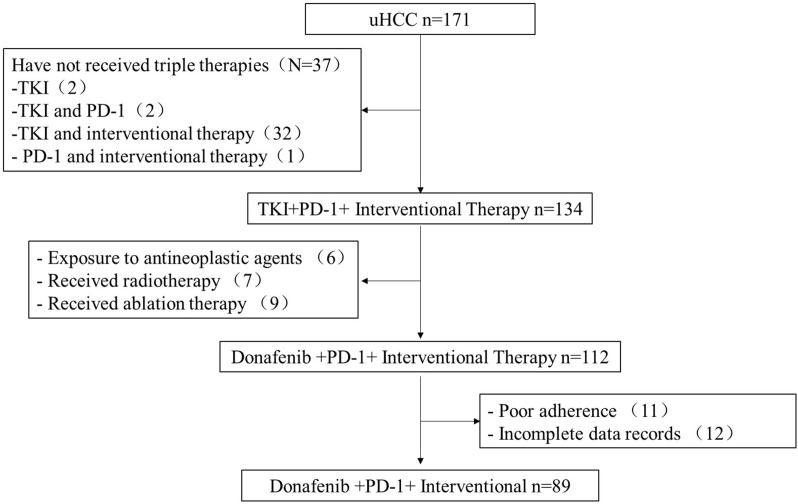
Methods: This retrospective study included 89 patients with uHCC who received donafenib, anti-PD-1 monoclonal antibodies (tislelizumab or sintilimab), and interventional therapies (TACE and/or HAIC) between March 2022 and December 2023. Outcomes included objective response rate (ORR), progression-free survival (PFS), overall survival (OS), and safety. Efficacy was assessed using modified RECIST (mRECIST) criteria; prognostic factors were analyzed using Cox regression models.
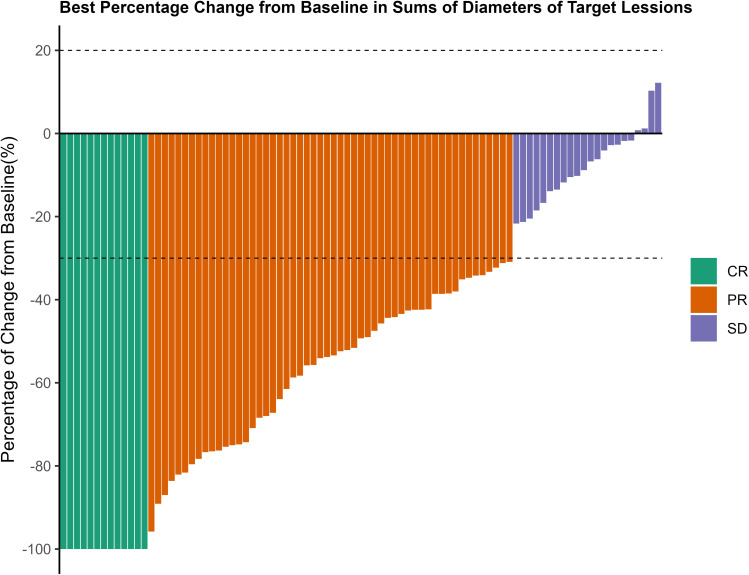
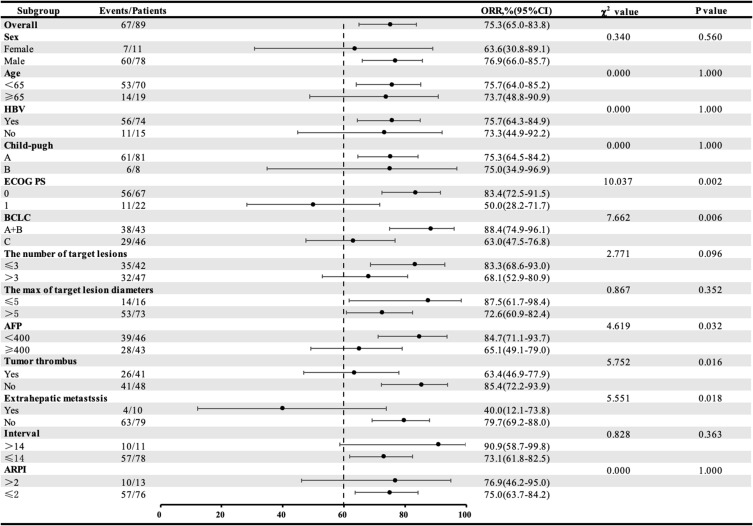
Results: Among 89 patients, the ORR was 75.3% and the disease control rate was 100%. The median PFS was 18.5 months (95% CI: 15.0-NA); median OS was not reached after a median follow-up of 13.7 months. PFS rates at 6, 12, and 18 months were 87.6%, 72.4%, and 52.7%, and OS rates were 93.3%, 81.6%, and 72.4%, respectively. Conversion surgery was achieved in 15.7% of patients. Subgroup analysis indicated that ECOG PS 1, extrahepatic metastases, and high baseline AFP were associated with worse survival outcomes, while interventional modality did not significantly affect prognosis. Multivariate analysis confirmed ECOG PS 1 and extrahepatic metastases as independent predictors of shorter PFS, and ECOG PS 1 and elevated AFP as independent predictors of worse OS. Grade ≥3 treatment-related adverse events occurred in 30.3% of patients; no treatment-related deaths were reported.
Conclusion: The combination of interventional therapies, donafenib, and anti-PD-1 monoclonal antibodies demonstrated promising efficacy and manageable safety in uHCC, warranting further validation in prospective trials.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


