Efficacy and Safety of the Multi-Level Comprehensive Collateral Artery Embolism Sequential Hepatic Arterial Infusion Chemotherapy, Combined with TKI and ICI, for Unresectable Huge Hepatocellular Carcinoma (>10cm): A Propensity Score Matching Cohort Study.
{"title":"Efficacy and Safety of the Multi-Level Comprehensive Collateral Artery Embolism Sequential Hepatic Arterial Infusion Chemotherapy, Combined with TKI and ICI, for Unresectable Huge Hepatocellular Carcinoma (>10cm): A Propensity Score Matching Cohort Study.","authors":"Hao-Yang Tan, Shuang-Quan Liu, Yan-Han Liu, Jiu-Ling Zheng, Hua-Guo Feng","doi":"10.2147/JHC.S546588","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This retrospective study was conducted to evaluate the effectiveness and safety of a new combination therapy of the multi-level comprehensive collateral artery embolism (CAE) sequential hepatic arterial infusion chemotherapy (HAIC), tyrosine kinase inhibitors (TKI) and immune checkpoint inhibitors (ICI) for unresectable huge hepatocellular carcinoma (>10cm) patients.</p><p><strong>Methods: </strong>A propensity score-matching (PSM) cohort study was conducted. The initial tumor response, treatment-related adverse events, and survival outcomes were compared. The Forestplot package was used to visualize and interpret forest plots of overall survival subgroup analyses. Univariate and multivariate analyses were conducted to explore the risk factors of overall survival.</p><p><strong>Results: </strong>Thirty-one pairs of patients were evaluated after PSM. There were statistically significant differences in the initial tumor response and objective response rate (ORR) between the two groups (74.2% vs 48.4%, P=0.037). Compared with the \"HAIC\" group, the incidence of abdominal pain was higher in the \"CAE+HAIC\" group (71.0% vs 41.9%, P=0.021). The OS and progression-free survival (PFS) of the \"CAE+HAIC\" group were longer than those of the \"HAIC\" group (OS: HR=0.439, 95% CI: 0.199-0.970, P=0.042; PFS: HR=0.475; 95% CI: 0.252-0.895; P=0.021). The CAE (HR=0.403, 95% CI: 0.213-0.762; P=0.005), prealbumin levels <170 mg/L (HR=2.195, 95% CI: 1.226-3.929; P=0.008), and lactic dehydrogenase levels >245 U/L (HR=2.136, 95% CI: 1.215-3.757; P=0.008) were independent risk factors of OS.</p><p><strong>Conclusions: </strong>The multi-level comprehensive CAE sequential HAIC, combined with TKI and ICI, can improve tumor response and prolong survival time in unresectable huge HCC patients while remaining safe and tolerable.</p>","PeriodicalId":15906,"journal":{"name":"Journal of Hepatocellular Carcinoma","volume":"12 ","pages":"1821-1834"},"PeriodicalIF":3.4000,"publicationDate":"2025-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12374706/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepatocellular Carcinoma","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/JHC.S546588","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: This retrospective study was conducted to evaluate the effectiveness and safety of a new combination therapy of the multi-level comprehensive collateral artery embolism (CAE) sequential hepatic arterial infusion chemotherapy (HAIC), tyrosine kinase inhibitors (TKI) and immune checkpoint inhibitors (ICI) for unresectable huge hepatocellular carcinoma (>10cm) patients.
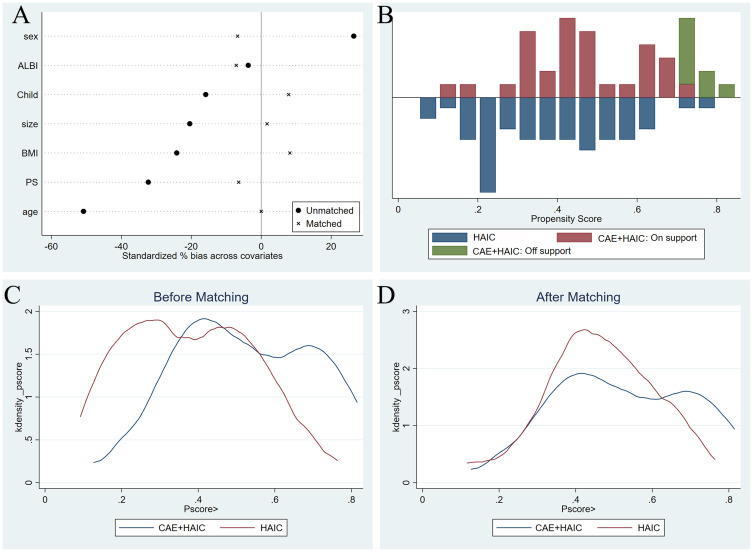
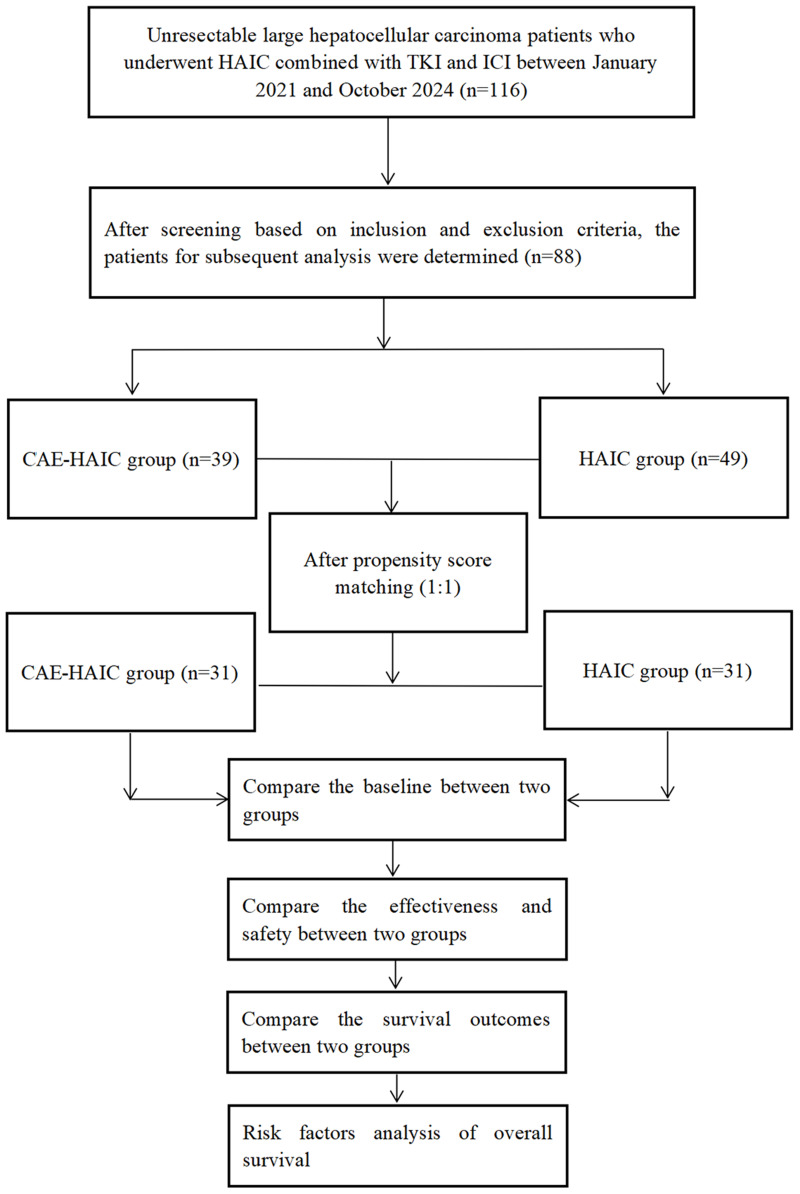
Methods: A propensity score-matching (PSM) cohort study was conducted. The initial tumor response, treatment-related adverse events, and survival outcomes were compared. The Forestplot package was used to visualize and interpret forest plots of overall survival subgroup analyses. Univariate and multivariate analyses were conducted to explore the risk factors of overall survival.
Results: Thirty-one pairs of patients were evaluated after PSM. There were statistically significant differences in the initial tumor response and objective response rate (ORR) between the two groups (74.2% vs 48.4%, P=0.037). Compared with the "HAIC" group, the incidence of abdominal pain was higher in the "CAE+HAIC" group (71.0% vs 41.9%, P=0.021). The OS and progression-free survival (PFS) of the "CAE+HAIC" group were longer than those of the "HAIC" group (OS: HR=0.439, 95% CI: 0.199-0.970, P=0.042; PFS: HR=0.475; 95% CI: 0.252-0.895; P=0.021). The CAE (HR=0.403, 95% CI: 0.213-0.762; P=0.005), prealbumin levels <170 mg/L (HR=2.195, 95% CI: 1.226-3.929; P=0.008), and lactic dehydrogenase levels >245 U/L (HR=2.136, 95% CI: 1.215-3.757; P=0.008) were independent risk factors of OS.
Conclusions: The multi-level comprehensive CAE sequential HAIC, combined with TKI and ICI, can improve tumor response and prolong survival time in unresectable huge HCC patients while remaining safe and tolerable.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


