Screening Candidates for Conversion Therapy in Unresectable Hepatocellular Carcinoma Patients After Tyrosine Kinase Inhibitor Plus PD-1/PD-L1 Antibody Therapy: A Multicenter Retrospective Study.
{"title":"Screening Candidates for Conversion Therapy in Unresectable Hepatocellular Carcinoma Patients After Tyrosine Kinase Inhibitor Plus PD-1/PD-L1 Antibody Therapy: A Multicenter Retrospective Study.","authors":"Zhe Jin, Xueyan Li, Ling Lv, Bin Zhang, Xiao Ma, Siqin Chen, Jingjing You, Xuewei Wu, Liaoyuan Wang, Xin Liu, Fei Wang, Xiaoming Chen, Lijuan Yu, Shuixing Zhang, Lu Zhang","doi":"10.2147/JHC.S523476","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Conversion therapies after immune checkpoint inhibitors (ICIs) plus tyrosine-kinase inhibitors (TKIs) provide curative surgery chance and prolong survival for unresectable hepatocellular carcinoma (uHCC). However, only some patients have the opportunity to receive conversion therapies. To this end, we aimed to develop and validate a machine-learning model to identify patients who may have the chance to undergo conversion therapy.</p><p><strong>Methods: </strong>This retrospective cohort study included 443 patients with uHCC who received ICIs and TKIs from four centers. Variables were analyzed using univariate and multivariate logistic regression to identify independent indicators of conversion therapy. The Gradient Boosting Machine (GBM) algorithm was used to develop and validate model, and the Shapley additive explanation algorithm was used to mechanically explain the prediction of the model.</p><p><strong>Results: </strong>Overall, 84 (19%) patients underwent conversion therapy, and their prognosis were significantly longer than those did not (<i>P</i> < 0.05). CA125 level, pre-TKI therapy, pre-antiviral therapy, lymph node metastasis status, and number of intrahepatic lesions were identified as indicators of conversion therapy. The GBM-based combined model outperformed the BCLC classification (<i>P</i> < 0.05), yielding an AUC of 0.76 and 0.74 in the training and external validation cohorts, respectively. Survival analyses indicated that patients who underwent surgery as conversion therapy had a better prognosis than those who underwent ablation therapy (<i>P</i> < 0.05).</p><p><strong>Conclusion: </strong>The GBM-based combined model could identify patients who may benefit from conversion therapy for uHCC treated with ICIs and TKIs. Surgical resection as curative conversion therapy may provide better survival benefits than ablation therapy.</p>","PeriodicalId":15906,"journal":{"name":"Journal of Hepatocellular Carcinoma","volume":"12 ","pages":"1921-1941"},"PeriodicalIF":3.4000,"publicationDate":"2025-08-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12396238/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepatocellular Carcinoma","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/JHC.S523476","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Conversion therapies after immune checkpoint inhibitors (ICIs) plus tyrosine-kinase inhibitors (TKIs) provide curative surgery chance and prolong survival for unresectable hepatocellular carcinoma (uHCC). However, only some patients have the opportunity to receive conversion therapies. To this end, we aimed to develop and validate a machine-learning model to identify patients who may have the chance to undergo conversion therapy.
Methods: This retrospective cohort study included 443 patients with uHCC who received ICIs and TKIs from four centers. Variables were analyzed using univariate and multivariate logistic regression to identify independent indicators of conversion therapy. The Gradient Boosting Machine (GBM) algorithm was used to develop and validate model, and the Shapley additive explanation algorithm was used to mechanically explain the prediction of the model.
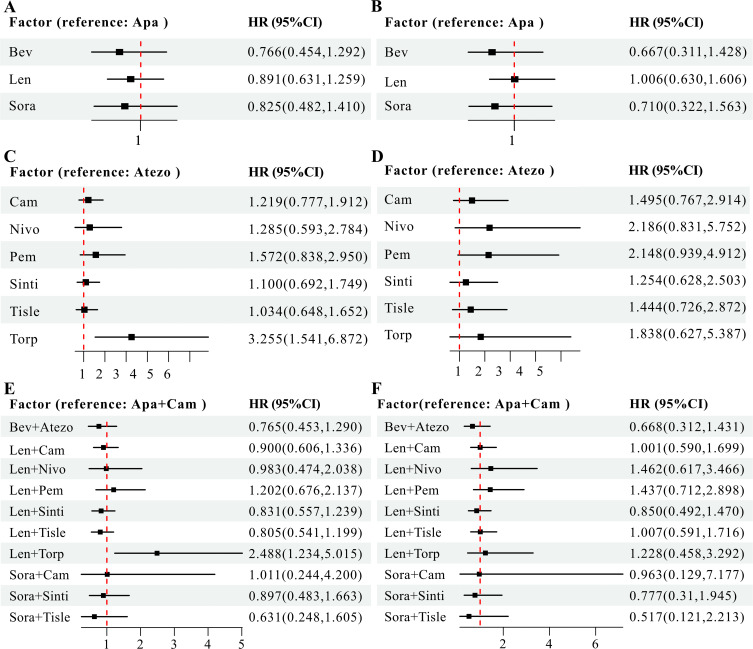
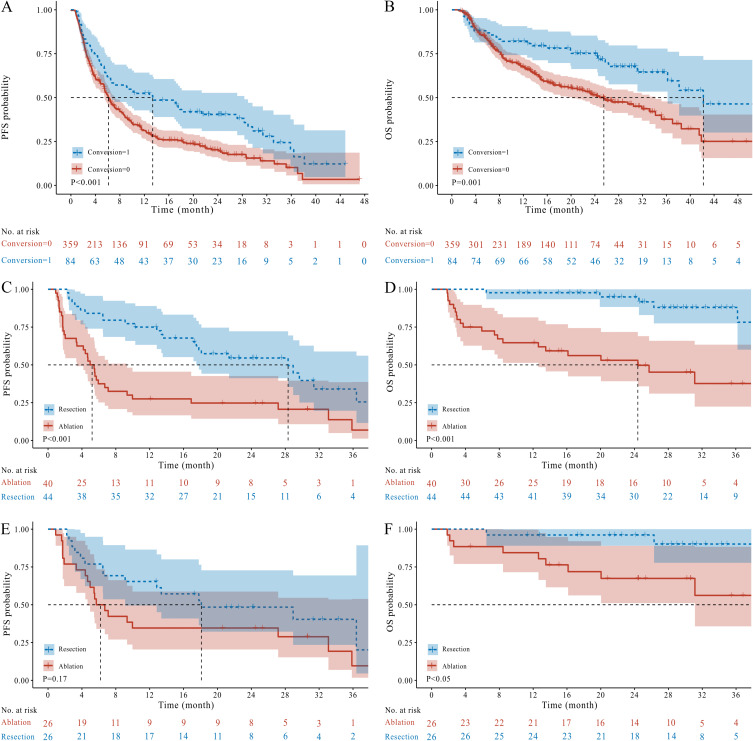
Results: Overall, 84 (19%) patients underwent conversion therapy, and their prognosis were significantly longer than those did not (P < 0.05). CA125 level, pre-TKI therapy, pre-antiviral therapy, lymph node metastasis status, and number of intrahepatic lesions were identified as indicators of conversion therapy. The GBM-based combined model outperformed the BCLC classification (P < 0.05), yielding an AUC of 0.76 and 0.74 in the training and external validation cohorts, respectively. Survival analyses indicated that patients who underwent surgery as conversion therapy had a better prognosis than those who underwent ablation therapy (P < 0.05).
Conclusion: The GBM-based combined model could identify patients who may benefit from conversion therapy for uHCC treated with ICIs and TKIs. Surgical resection as curative conversion therapy may provide better survival benefits than ablation therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


