{"title":"PO-llution control: a cross-sectional study on the role of antimicrobial stewardship in reducing healthcare's carbon footprint.","authors":"Saied Ali, Sadhbh Gash, Niamh Weir, Karen Burns, Binu Dinesh, Helene Mcdermott, Fidelma Fitzpatrick, Sinead O'Donnell, Ciara O'Connor","doi":"10.1093/jacamr/dlaf146","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To evaluate the environmental impact of prolonged IV antimicrobial courses and identify opportunities for improved antimicrobial stewardship (AMS) practices.</p><p><strong>Methods: </strong>A retrospective cross-sectional study was conducted using AMS ward-round data from January 2023 to December 2024 at a tertiary hospital in Dublin, Ireland. Data on IV antimicrobial prescriptions, AMS recommendations for discontinuation or IV to oral switch (IVOS) and prescriber acceptance were reviewed. A life cycle assessment, informed by published literature, was used to estimate the carbon footprint associated with IV use.</p><p><strong>Results: </strong>Of 1929 antimicrobial prescriptions reviewed, 58% (<i>n</i> = 1119) were being administered IV. Among 435 IV prescriptions with AMS, recommendations to stop (<i>n</i> = 357) or IVOS (<i>n</i> = 78), 229 (52.6%) were accepted, resulting in a reduction of 106.5 kg of clinical waste and 261.2 kg carbon dioxide equivalents (CO₂e) emissions. The remaining 206 IV prescriptions (47.4%) were categorized as prolonged IV prescriptions, generating 98.8 kg of clinical waste and 245.8 kg CO₂e; averaging 0.48 kg of waste and 1.19 kg CO₂e per prescription. To contextualize, the carbon footprint of each prolonged prescription equates to driving 6.2 km, performing 10 chest X-rays or operating a 10 W light-emitting diode bulb continuously for 1200 h. Piperacillin-tazobactam, amoxicillin-clavulanic acid, cefuroxime, metronidazole and meropenem together accounted for over 84% of total emissions, with piperacillin-tazobactam alone contributing 97.5 kg CO₂e and 41.6 kg of waste from 62 prolonged prescriptions.</p><p><strong>Conclusions: </strong>In addition to patient safety risks, prolonged IV antimicrobial courses generate considerable environmental waste. Aligning AMS with sustainability goals may contribute to addressing the dual crises of antimicrobial resistance and climate change.</p>","PeriodicalId":14594,"journal":{"name":"JAC-Antimicrobial Resistance","volume":"7 4","pages":"dlaf146"},"PeriodicalIF":3.3000,"publicationDate":"2025-08-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12391753/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAC-Antimicrobial Resistance","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jacamr/dlaf146","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To evaluate the environmental impact of prolonged IV antimicrobial courses and identify opportunities for improved antimicrobial stewardship (AMS) practices.
Methods: A retrospective cross-sectional study was conducted using AMS ward-round data from January 2023 to December 2024 at a tertiary hospital in Dublin, Ireland. Data on IV antimicrobial prescriptions, AMS recommendations for discontinuation or IV to oral switch (IVOS) and prescriber acceptance were reviewed. A life cycle assessment, informed by published literature, was used to estimate the carbon footprint associated with IV use.
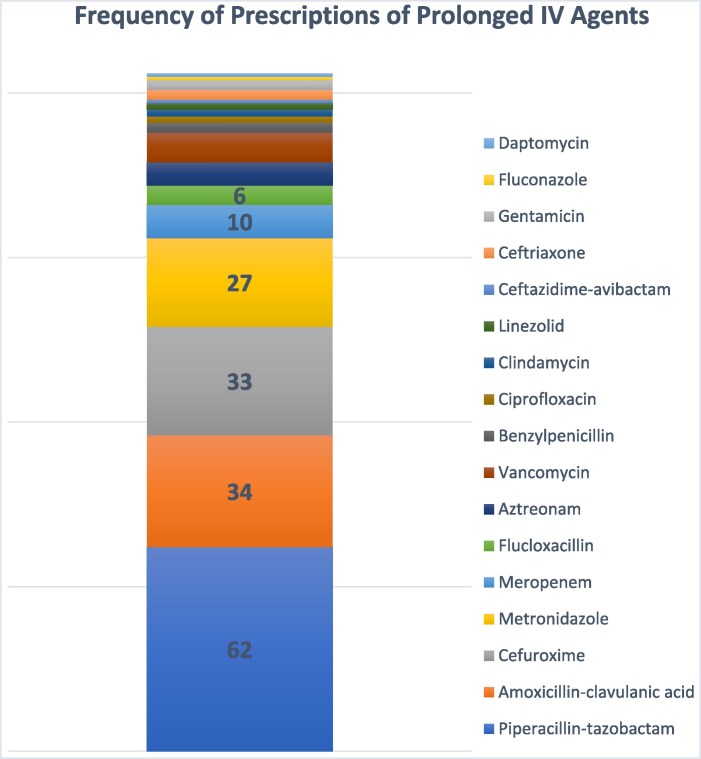
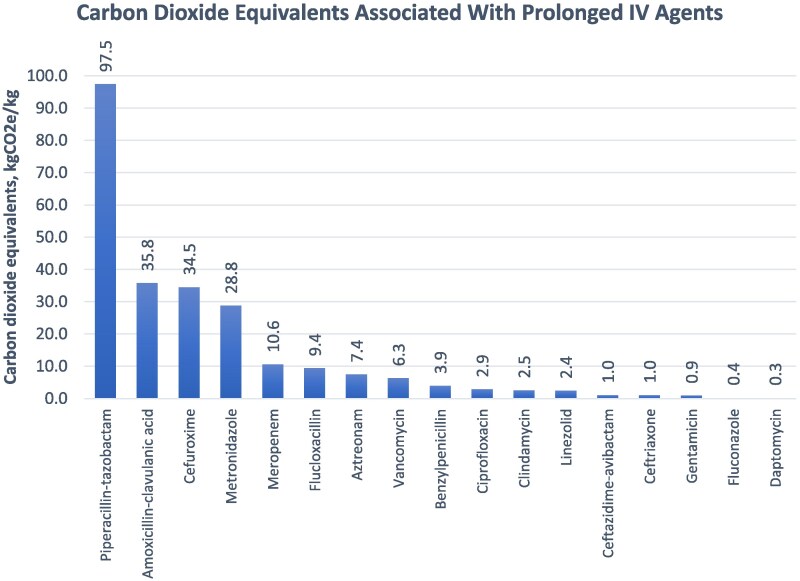
Results: Of 1929 antimicrobial prescriptions reviewed, 58% (n = 1119) were being administered IV. Among 435 IV prescriptions with AMS, recommendations to stop (n = 357) or IVOS (n = 78), 229 (52.6%) were accepted, resulting in a reduction of 106.5 kg of clinical waste and 261.2 kg carbon dioxide equivalents (CO₂e) emissions. The remaining 206 IV prescriptions (47.4%) were categorized as prolonged IV prescriptions, generating 98.8 kg of clinical waste and 245.8 kg CO₂e; averaging 0.48 kg of waste and 1.19 kg CO₂e per prescription. To contextualize, the carbon footprint of each prolonged prescription equates to driving 6.2 km, performing 10 chest X-rays or operating a 10 W light-emitting diode bulb continuously for 1200 h. Piperacillin-tazobactam, amoxicillin-clavulanic acid, cefuroxime, metronidazole and meropenem together accounted for over 84% of total emissions, with piperacillin-tazobactam alone contributing 97.5 kg CO₂e and 41.6 kg of waste from 62 prolonged prescriptions.
Conclusions: In addition to patient safety risks, prolonged IV antimicrobial courses generate considerable environmental waste. Aligning AMS with sustainability goals may contribute to addressing the dual crises of antimicrobial resistance and climate change.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


