The effect of intraoperative excessive bleeding on the pharmacokinetics of ampicillin and sulbactam in recipients of living donor liver transplantation in Japan.
{"title":"The effect of intraoperative excessive bleeding on the pharmacokinetics of ampicillin and sulbactam in recipients of living donor liver transplantation in Japan.","authors":"Yuji Wakimoto, Koh Okamoto, Takehito Yamamoto, Nobuhisa Akamatsu, Taro Kariya, Yoko Hoshino, Sohei Harada, Hideki Hashimoto, Daisuke Jubishi, Takehiro Tanaka, Ryo Yamaguchi, Junichi Kaneko, Shu Okugawa, Tappei Takada, Kiyoshi Hasegawa, Kanji Uchida, Takeya Tsutsumi","doi":"10.1093/jacamr/dlaf149","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Guidelines recommend redosing with intravenous prophylactic antibiotics when excessive bleeding exceeds 1500 mL during surgery based on the pharmacokinetics data of cefazolin. However, the necessity for redosing of other antibiotics and the threshold volume of blood loss necessitating such supplementation remain undefined. We investigated plasma antibiotic concentrations during liver transplant surgery in patients with frequent excessive bleeding.</p><p><strong>Methods: </strong>A single-centre, prospective, observational pharmacokinetic study was conducted. Adult liver transplant recipients who received 2 g of ampicillin and 1 g of sulbactam every 3 h during surgery were included. Blood samples were collected hourly during surgery, and intraoperative bleeding amounts were reviewed from anaesthesia records. Plasma concentrations of ampicillin and sulbactam were determined using validated liquid chromatography-tandem mass spectrometry. The probability of target attainment was set at 80% free time above the MIC (fT > MIC).</p><p><strong>Results: </strong>Twenty participants were included. Of these, 11 participants (55%) were female. The median age, body weight, and bleeding volume were 52 years, 62.1 kg, and 11 158 mL, respectively. The intraoperative clearance of ampicillin was 80.28 mL/min, and sulbactam was 77.23 mL/min. The fT > MIC for both ampicillin and sulbactam tended to be lower with bleeding > 20 000 mL than with less bleeding. Plasma concentrations of ampicillin and sulbactam were maintained during surgery without redosing, even after bleeding exceeded 1500 mL.</p><p><strong>Conclusions: </strong>Even with excessive bleeding, administering 3 g of ampicillin/sulbactam every 3 h maintained sufficient plasma concentration. Redosing may be unnecessary unless total bleeding exceeds 20 000 mL.</p>","PeriodicalId":14594,"journal":{"name":"JAC-Antimicrobial Resistance","volume":"7 4","pages":"dlaf149"},"PeriodicalIF":3.3000,"publicationDate":"2025-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12378435/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAC-Antimicrobial Resistance","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jacamr/dlaf149","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Guidelines recommend redosing with intravenous prophylactic antibiotics when excessive bleeding exceeds 1500 mL during surgery based on the pharmacokinetics data of cefazolin. However, the necessity for redosing of other antibiotics and the threshold volume of blood loss necessitating such supplementation remain undefined. We investigated plasma antibiotic concentrations during liver transplant surgery in patients with frequent excessive bleeding.
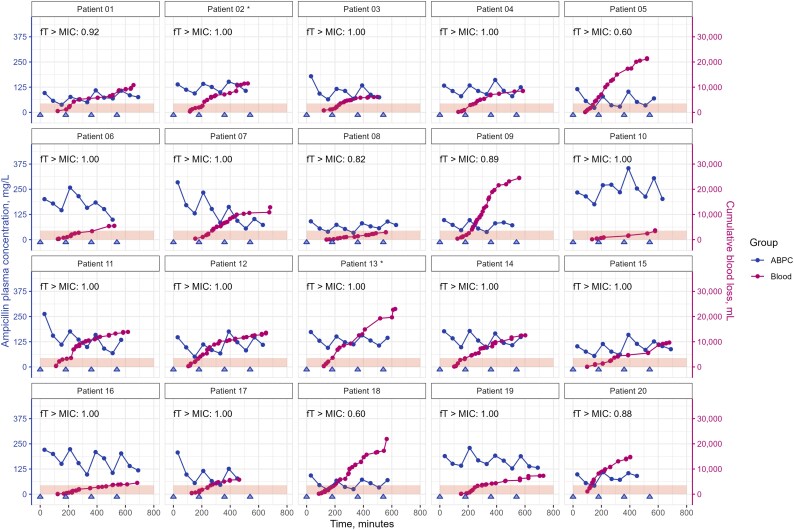
Methods: A single-centre, prospective, observational pharmacokinetic study was conducted. Adult liver transplant recipients who received 2 g of ampicillin and 1 g of sulbactam every 3 h during surgery were included. Blood samples were collected hourly during surgery, and intraoperative bleeding amounts were reviewed from anaesthesia records. Plasma concentrations of ampicillin and sulbactam were determined using validated liquid chromatography-tandem mass spectrometry. The probability of target attainment was set at 80% free time above the MIC (fT > MIC).
Results: Twenty participants were included. Of these, 11 participants (55%) were female. The median age, body weight, and bleeding volume were 52 years, 62.1 kg, and 11 158 mL, respectively. The intraoperative clearance of ampicillin was 80.28 mL/min, and sulbactam was 77.23 mL/min. The fT > MIC for both ampicillin and sulbactam tended to be lower with bleeding > 20 000 mL than with less bleeding. Plasma concentrations of ampicillin and sulbactam were maintained during surgery without redosing, even after bleeding exceeded 1500 mL.
Conclusions: Even with excessive bleeding, administering 3 g of ampicillin/sulbactam every 3 h maintained sufficient plasma concentration. Redosing may be unnecessary unless total bleeding exceeds 20 000 mL.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


