Brigitta Y M van der Kolk, Gaby J van den Wittenboer, Ingrid M Nijholt, Martin Podlogar, Wimar A van den Brink, Gerrit Joan Bouma, Lonneke N Buijteweg, Boudewijn A A M van Hasselt, Niels W L Schep, Mario Maas, Martijn F Boomsma
{"title":"Determining the need for stabilising therapy of cervical spine injuries on CT: towards standardising decision-making in the emergency department.","authors":"Brigitta Y M van der Kolk, Gaby J van den Wittenboer, Ingrid M Nijholt, Martin Podlogar, Wimar A van den Brink, Gerrit Joan Bouma, Lonneke N Buijteweg, Boudewijn A A M van Hasselt, Niels W L Schep, Mario Maas, Martijn F Boomsma","doi":"10.1186/s12245-025-00965-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In clinical practice, currently no standardised approach exists to determine which patients with cervical spine injury (CSI) on CT scan should receive continued cervical spine immobilisation and a neurosurgeon is generally consulted. Insights into the contribution of CT assessment and classification of CSI in determining the need for stabilising therapy could aid in standardising clinical practice in the emergency department. Standardising clinical practice for cervical spine immobilisation could potentially improve the patient flow in the emergency department by reducing delay in decision-making, particularly in hospitals without availability of immediate neurosurgical consultation. Therefore the aim of this study was to investigate if CT assessment and classification of CSI, without clinical information, can determine whether a patients' injury is an injury in need of stabilising therapy (IST).</p><p><strong>Methods: </strong>In this observational, retrospective study, a database with a multidisciplinary, extensively validated reference standard was used. Consecutive patients screened for CSI using CT (2007-2014) in a level-one trauma centre in the Netherlands were included. Actual therapy that has been provided was compared to the assessment of CSI by three neurosurgeons on CT for presence of ISTs. Clinical information was not provided during initial CT assessment. Injury types were classified according to the AOSpine Injury Classification System. Concordance rates of CT assessment by the neurosurgeons compared to actual therapy provided for presence of ISTs with 95% confidence intervals (95% CI) were calculated.</p><p><strong>Results: </strong>Of the 273 patients in the database with a CSI, 262 were included. CT assessment of CSIs led to assignment as IST in 155/262 cases (59.2%). Based on the actual therapy provided, 124/262 cases (47.3%) were an IST. CT assessment by the neurosurgeons was concordant with the therapy provided for presence of ISTs in 91.9% [95% CI 85.3-95.9%], and for absence of ISTs in 70.3% [95% CI 61.8-77.6%]. After allocation of the AO-subtypes to IST and non-IST, 168/171 (98.2%) of A0-injury subtype cases were non-IST.</p><p><strong>Conclusion: </strong>CT scan assessment and injury classification without clinical information allows identification of most injuries in need of stabilising therapy, with a low miss rate of ISTs, particularly for the A0-injury subtype.</p>","PeriodicalId":13967,"journal":{"name":"International Journal of Emergency Medicine","volume":"18 1","pages":"159"},"PeriodicalIF":2.0000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12382177/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s12245-025-00965-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In clinical practice, currently no standardised approach exists to determine which patients with cervical spine injury (CSI) on CT scan should receive continued cervical spine immobilisation and a neurosurgeon is generally consulted. Insights into the contribution of CT assessment and classification of CSI in determining the need for stabilising therapy could aid in standardising clinical practice in the emergency department. Standardising clinical practice for cervical spine immobilisation could potentially improve the patient flow in the emergency department by reducing delay in decision-making, particularly in hospitals without availability of immediate neurosurgical consultation. Therefore the aim of this study was to investigate if CT assessment and classification of CSI, without clinical information, can determine whether a patients' injury is an injury in need of stabilising therapy (IST).
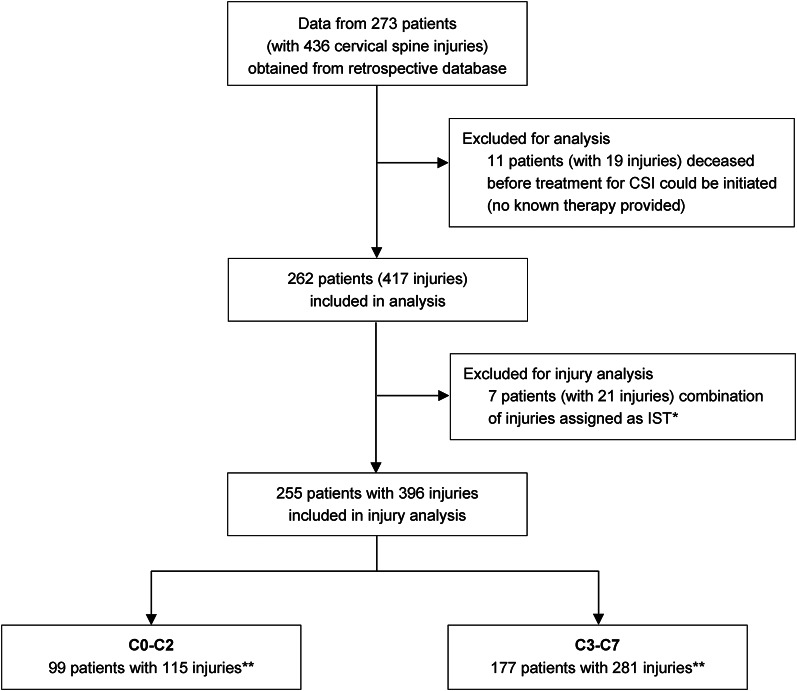
Methods: In this observational, retrospective study, a database with a multidisciplinary, extensively validated reference standard was used. Consecutive patients screened for CSI using CT (2007-2014) in a level-one trauma centre in the Netherlands were included. Actual therapy that has been provided was compared to the assessment of CSI by three neurosurgeons on CT for presence of ISTs. Clinical information was not provided during initial CT assessment. Injury types were classified according to the AOSpine Injury Classification System. Concordance rates of CT assessment by the neurosurgeons compared to actual therapy provided for presence of ISTs with 95% confidence intervals (95% CI) were calculated.
Results: Of the 273 patients in the database with a CSI, 262 were included. CT assessment of CSIs led to assignment as IST in 155/262 cases (59.2%). Based on the actual therapy provided, 124/262 cases (47.3%) were an IST. CT assessment by the neurosurgeons was concordant with the therapy provided for presence of ISTs in 91.9% [95% CI 85.3-95.9%], and for absence of ISTs in 70.3% [95% CI 61.8-77.6%]. After allocation of the AO-subtypes to IST and non-IST, 168/171 (98.2%) of A0-injury subtype cases were non-IST.
Conclusion: CT scan assessment and injury classification without clinical information allows identification of most injuries in need of stabilising therapy, with a low miss rate of ISTs, particularly for the A0-injury subtype.
期刊介绍:
The aim of the journal is to bring to light the various clinical advancements and research developments attained over the world and thus help the specialty forge ahead. It is directed towards physicians and medical personnel undergoing training or working within the field of Emergency Medicine. Medical students who are interested in pursuing a career in Emergency Medicine will also benefit from the journal. This is particularly useful for trainees in countries where the specialty is still in its infancy. Disciplines covered will include interesting clinical cases, the latest evidence-based practice and research developments in Emergency medicine including emergency pediatrics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


