Different underlying aetiologies in patients presenting with ventricular tachycardia fulfilling task force criteria for arrhythmogenic right ventricular cardiomyopathy: initial suspicion based on the 12-lead electrocardiogram.
Jarieke C Hoogendoorn, Laurens P Bosman, Jeroen F van der Heijden, Arthur A Wilde, Maarten P van den Berg, Sing-Chien Yap, J Peter van Tintelen, Dennis Dooijes, Anneline S J M Te Riele, Katja Zeppenfeld
{"title":"Different underlying aetiologies in patients presenting with ventricular tachycardia fulfilling task force criteria for arrhythmogenic right ventricular cardiomyopathy: initial suspicion based on the 12-lead electrocardiogram.","authors":"Jarieke C Hoogendoorn, Laurens P Bosman, Jeroen F van der Heijden, Arthur A Wilde, Maarten P van den Berg, Sing-Chien Yap, J Peter van Tintelen, Dennis Dooijes, Anneline S J M Te Riele, Katja Zeppenfeld","doi":"10.1093/europace/euaf136","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The task force criteria (TFC) for arrhythmogenic right ventricular cardiomyopathy (ARVC) are highly sensitive but lack specificity. Atypical RV involvement (aRVi) may indicate different underlying aetiologies and prognosis, requiring specific therapeutic interventions. We aimed to evaluate the role of the baseline 12-lead ECG for initial suspicion of aRVi.</p><p><strong>Methods: </strong>From the Netherlands Heart Institute Arrhythmogenic Cardiomyopathy (NHI-ACM) registry, patients were selected who (i) fulfilled TFC for definite ARVC, (ii) presented with sustained ventricular tachycardia (VT), and (iii) underwent genetic testing. The first available ECG after VT was evaluated. PR prolongation ≥220 ms and/or a surface area of the maximum R'-wave in V1-V3 of ≥1.65 mm2 was defined as an aRVi-ECG. Patients with an ARVC-related pathogenic/likely pathogenic variant (P/LP+) were classified as 'ARVC'. Data of P/LP- were reviewed by an expert panel and classified as either 'ARVC' or 'different aetiology' based on consensus.</p><p><strong>Results: </strong>A total of 159 patients were included (122 P/LP+ and 37 P/LP- patients). Nineteen patients had an aRVi-ECG [11 (9%) P/LP+ vs. 8 (22%) P/LP-, P = 0.038]. Of the P/LP- patients, 17 (46%) were classified as 'different aetiology' (e.g. myocarditis, ischaemia, sarcoidosis), including all 8 patients with an aRVi-ECG. Among the P/LP+ patients with an aRVi-ECG, 46% carried the p.Arg14del phospholamban pathogenic variant, and 64% died compared to 15 and 19% of P/LP+ patients without an aRVi-ECG, respectively (both P < 0.01).</p><p><strong>Conclusion: </strong>In P/LP- patients presenting with VT and fulfilling TFC, an aRVi-ECG should raise suspicion for a different underlying aetiology. In P/LP+ patients, an aRVi-ECG may identify those with poor outcome.</p>","PeriodicalId":11981,"journal":{"name":"Europace","volume":"27 8","pages":""},"PeriodicalIF":7.4000,"publicationDate":"2025-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12365759/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Europace","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/europace/euaf136","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
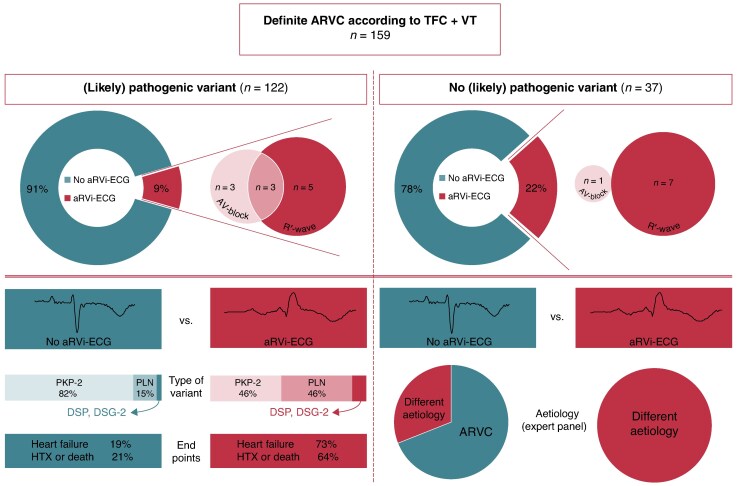
Aims: The task force criteria (TFC) for arrhythmogenic right ventricular cardiomyopathy (ARVC) are highly sensitive but lack specificity. Atypical RV involvement (aRVi) may indicate different underlying aetiologies and prognosis, requiring specific therapeutic interventions. We aimed to evaluate the role of the baseline 12-lead ECG for initial suspicion of aRVi.
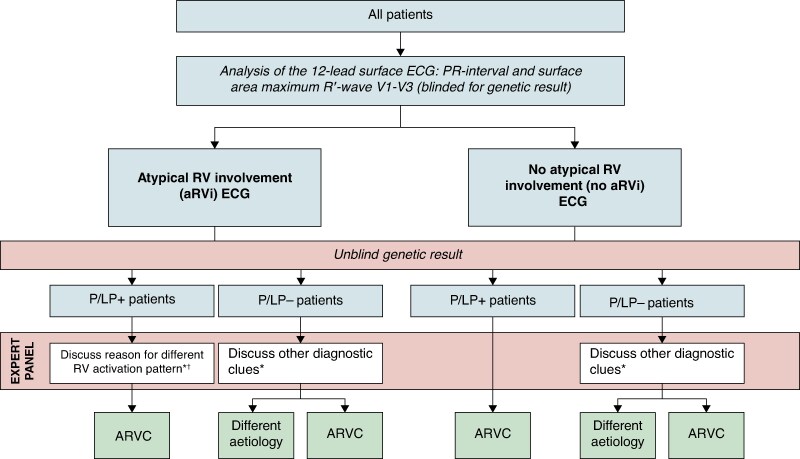
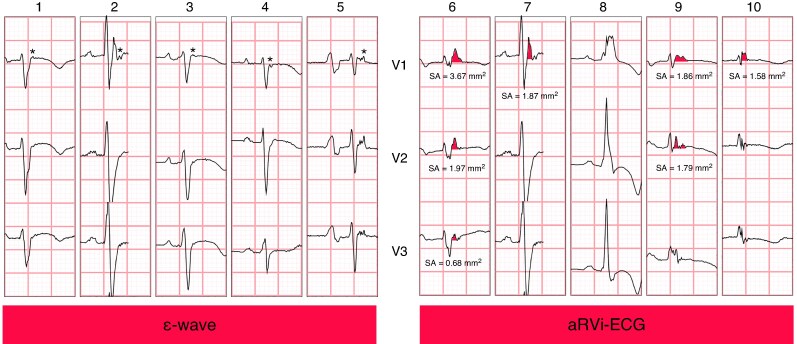
Methods: From the Netherlands Heart Institute Arrhythmogenic Cardiomyopathy (NHI-ACM) registry, patients were selected who (i) fulfilled TFC for definite ARVC, (ii) presented with sustained ventricular tachycardia (VT), and (iii) underwent genetic testing. The first available ECG after VT was evaluated. PR prolongation ≥220 ms and/or a surface area of the maximum R'-wave in V1-V3 of ≥1.65 mm2 was defined as an aRVi-ECG. Patients with an ARVC-related pathogenic/likely pathogenic variant (P/LP+) were classified as 'ARVC'. Data of P/LP- were reviewed by an expert panel and classified as either 'ARVC' or 'different aetiology' based on consensus.
Results: A total of 159 patients were included (122 P/LP+ and 37 P/LP- patients). Nineteen patients had an aRVi-ECG [11 (9%) P/LP+ vs. 8 (22%) P/LP-, P = 0.038]. Of the P/LP- patients, 17 (46%) were classified as 'different aetiology' (e.g. myocarditis, ischaemia, sarcoidosis), including all 8 patients with an aRVi-ECG. Among the P/LP+ patients with an aRVi-ECG, 46% carried the p.Arg14del phospholamban pathogenic variant, and 64% died compared to 15 and 19% of P/LP+ patients without an aRVi-ECG, respectively (both P < 0.01).
Conclusion: In P/LP- patients presenting with VT and fulfilling TFC, an aRVi-ECG should raise suspicion for a different underlying aetiology. In P/LP+ patients, an aRVi-ECG may identify those with poor outcome.
期刊介绍:
EP - Europace - European Journal of Pacing, Arrhythmias and Cardiac Electrophysiology of the European Heart Rhythm Association of the European Society of Cardiology. The journal aims to provide an avenue of communication of top quality European and international original scientific work and reviews in the fields of Arrhythmias, Pacing and Cellular Electrophysiology. The Journal offers the reader a collection of contemporary original peer-reviewed papers, invited papers and editorial comments together with book reviews and correspondence.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


