Stéphane Jouneau, Pierre Chauvin, Mathieu Lederlin, Benoît Painvin, Mallorie Kerjouan
{"title":"Pharmacotherapy for Autoimmune Pulmonary Alveolar Proteinosis.","authors":"Stéphane Jouneau, Pierre Chauvin, Mathieu Lederlin, Benoît Painvin, Mallorie Kerjouan","doi":"10.1007/s40265-025-02228-3","DOIUrl":null,"url":null,"abstract":"<p><p>Pulmonary alveolar proteinosis is suspected when a \"crazy paving\" pattern is observed on a chest CT scan. This diagnosis is confirmed by the presence of eosinophilic extracellular material that shows positive staining with Periodic Acid Schiff on bronchoalveolar lavage samples. The autoimmune form of pulmonary alveolar proteinosis is confirmed by detecting anti-granulocyte-macrophage colony-stimulating factor antibodies in the patient's serum. The historical first-line treatment for autoimmune pulmonary alveolar proteinosis is whole lung lavage, which should only be performed in expert centers. It remains the preferred treatment for patients experiencing respiratory failure, especially at the time of diagnosis. Inhaled granulocyte-macrophage colony-stimulating factor supplementation with molgramostim or sargramostim is now considered a first-line treatment in the international guidelines for autoimmune pulmonary alveolar proteinosis, following the positive results of recent randomized placebo-controlled studies. Rituximab and plasmapheresis can be prescribed as third- and fourth-line treatments, respectively. Lung transplantation may be considered for eligible patients experiencing terminal respiratory failure. A deeper understanding of the pathogenesis of autoimmune pulmonary alveolar proteinosis has opened up new therapeutic avenues, such as the use of PPARγ agonists or statins.</p>","PeriodicalId":11482,"journal":{"name":"Drugs","volume":" ","pages":"1193-1206"},"PeriodicalIF":14.4000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12484331/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drugs","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40265-025-02228-3","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/27 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
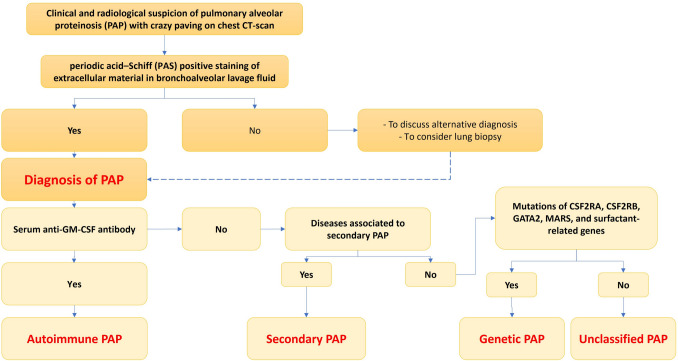
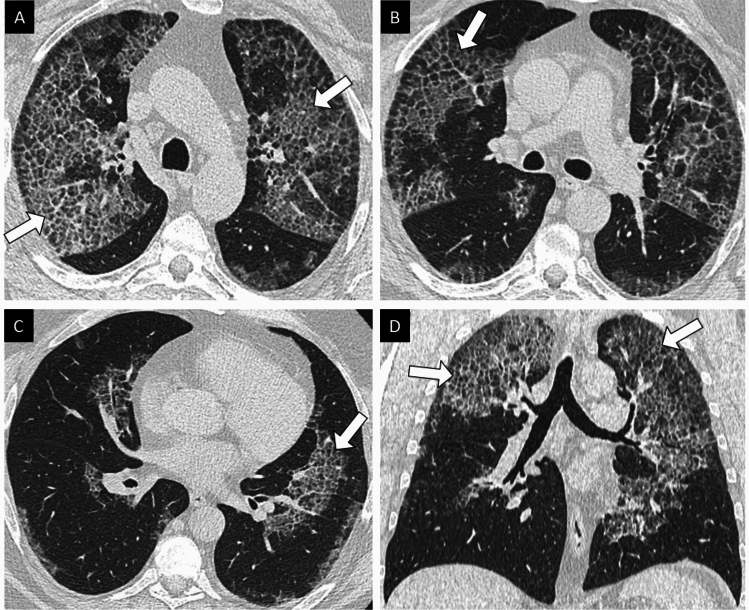
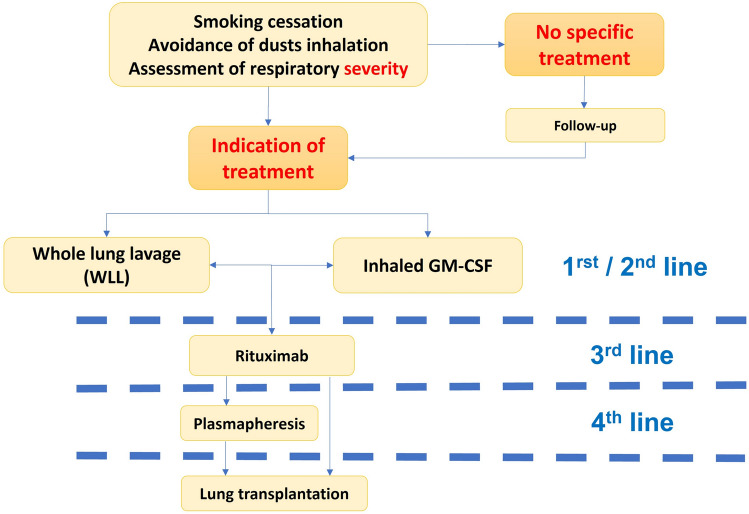
Pulmonary alveolar proteinosis is suspected when a "crazy paving" pattern is observed on a chest CT scan. This diagnosis is confirmed by the presence of eosinophilic extracellular material that shows positive staining with Periodic Acid Schiff on bronchoalveolar lavage samples. The autoimmune form of pulmonary alveolar proteinosis is confirmed by detecting anti-granulocyte-macrophage colony-stimulating factor antibodies in the patient's serum. The historical first-line treatment for autoimmune pulmonary alveolar proteinosis is whole lung lavage, which should only be performed in expert centers. It remains the preferred treatment for patients experiencing respiratory failure, especially at the time of diagnosis. Inhaled granulocyte-macrophage colony-stimulating factor supplementation with molgramostim or sargramostim is now considered a first-line treatment in the international guidelines for autoimmune pulmonary alveolar proteinosis, following the positive results of recent randomized placebo-controlled studies. Rituximab and plasmapheresis can be prescribed as third- and fourth-line treatments, respectively. Lung transplantation may be considered for eligible patients experiencing terminal respiratory failure. A deeper understanding of the pathogenesis of autoimmune pulmonary alveolar proteinosis has opened up new therapeutic avenues, such as the use of PPARγ agonists or statins.
期刊介绍:
Drugs is a journal that aims to enhance pharmacotherapy by publishing review and original research articles on key aspects of clinical pharmacology and therapeutics. The journal includes:
Leading/current opinion articles providing an overview of contentious or emerging issues.
Definitive reviews of drugs and drug classes, and their place in disease management.
Therapy in Practice articles including recommendations for specific clinical situations.
High-quality, well designed, original clinical research.
Adis Drug Evaluations reviewing the properties and place in therapy of both newer and established drugs.
AdisInsight Reports summarising development at first global approval.
Moreover, the journal offers additional digital features such as animated abstracts, video abstracts, instructional videos, and podcasts to increase visibility and educational value. Plain language summaries accompany articles to assist readers with some knowledge of the field in understanding important medical advances.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


