Supplemental parenteral nutrition within an enhanced recovery program for open pancreatoduodenectomy for cancer: a pragmatic, multicenter, randomized controlled trial.
Luca Gianotti, Salvatore Paiella, Giovanni Capretti, Nicolò Pecorelli, Isabella Frigerio, Marta Sandini, Alessandro Fogliati, Eleonora Vico, Marco Braga, Christian Cotsoglou, Alfonso Pedalino, Giuseppe Malleo, Simone Ricchitelli, Sabrina Caspani, Giovanni Guarneri, Alessia Vallorani, Alessandro Giardino, Elettra Pasqualoni, Roberto Salvia, Alessandro Zerbi, Massimo Falconi, Giovanni Butturini, Davide Paolo Bernasconi
{"title":"Supplemental parenteral nutrition within an enhanced recovery program for open pancreatoduodenectomy for cancer: a pragmatic, multicenter, randomized controlled trial.","authors":"Luca Gianotti, Salvatore Paiella, Giovanni Capretti, Nicolò Pecorelli, Isabella Frigerio, Marta Sandini, Alessandro Fogliati, Eleonora Vico, Marco Braga, Christian Cotsoglou, Alfonso Pedalino, Giuseppe Malleo, Simone Ricchitelli, Sabrina Caspani, Giovanni Guarneri, Alessia Vallorani, Alessandro Giardino, Elettra Pasqualoni, Roberto Salvia, Alessandro Zerbi, Massimo Falconi, Giovanni Butturini, Davide Paolo Bernasconi","doi":"10.1016/j.eclinm.2025.103455","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The role of supplemental parenteral nutrition (SPN) following pancreatoduodenectomy (PD) in the context of an enhanced recovery program is unexplored. This study aimed to determine whether SPN is superior to early oral feeding alone in reducing postoperative complications.</p><p><strong>Methods: </strong>This pragmatic, multicenter, randomized controlled, trial, across five centers in Italy, enrolled patients aged 18-89 years undergoing open PD for cancer. We excluded patients with an American Society of Anaesthesiology physical status >3 and a preoperative body weight loss of ≥15%. Patients were randomly assigned (1:1) postoperatively to either SPN from day 1 to 5 or no-SPN. All patients were free to begin oral feeding after the operation as desired in the context of a full enhanced recovery after surgery (ERAS) program. The primary outcome was morbidity burden, measured using the comprehensive complication index (CCI). Secondary outcomes included the overall rate of morbidity. Outcomes were assessed up to 90 days postoperatively. Overall, 120 patients per group were required to achieve 80% power and detect at least 30% reduction in the CCI in the SPN group, which was expected to be 23 (median) (interquartile range 21-31). The expected complication rate was 60%, and the type I error rate was set at 5%. Registration at ClinicalTrials.gov (#NCT04438447).</p><p><strong>Findings: </strong>From June 1, 2022, to December 20, 2023, 405 patients were screened for eligibility and 254 patients were randomly allocated to control (no-SPN; n = 129) or treatment (SPN; n = 125) group. All patients were included in the primary and secondary outcome analysis according to the intent-to-treat principle. The median CCI was 20.9 in both arms (median difference 0 [95% CI: -1.07 to 1.7]). The proportion of patients with at least one complication (CCI >0) was similar in both groups [(29.6% vs 29.2%; risk difference 0.4 (95% CI -11.1 to 7.0)]. The overall 90-day morbidity was 67.4% and 63.2% in the no-SPN arm and SPN arm groups, respectively [risk difference -4.2 (95% CI -16.7 to 8.2)]. In high nutritional risk patients (nutritional risk score ≥3), SPN was not protective against the primary outcome when compared with low-risk patients [OR 1.16 (95% CI 0.71-1.91)].</p><p><strong>Interpretation: </strong>In an ERAS program emphasizing early postoperative oral feeding, SPN does not affect outcome measures, even in patients at high nutritional risk. However, these results do not apply to severely malnourished patients or with critical comorbidities.</p><p><strong>Funding: </strong>The Italian Society for Artificial Nutrition and Metabolism (SINPE) and Baxter Italia S.p.A (Rome, Italy).</p>","PeriodicalId":11393,"journal":{"name":"EClinicalMedicine","volume":"87 ","pages":"103455"},"PeriodicalIF":10.0000,"publicationDate":"2025-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12396495/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"EClinicalMedicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.eclinm.2025.103455","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The role of supplemental parenteral nutrition (SPN) following pancreatoduodenectomy (PD) in the context of an enhanced recovery program is unexplored. This study aimed to determine whether SPN is superior to early oral feeding alone in reducing postoperative complications.
Methods: This pragmatic, multicenter, randomized controlled, trial, across five centers in Italy, enrolled patients aged 18-89 years undergoing open PD for cancer. We excluded patients with an American Society of Anaesthesiology physical status >3 and a preoperative body weight loss of ≥15%. Patients were randomly assigned (1:1) postoperatively to either SPN from day 1 to 5 or no-SPN. All patients were free to begin oral feeding after the operation as desired in the context of a full enhanced recovery after surgery (ERAS) program. The primary outcome was morbidity burden, measured using the comprehensive complication index (CCI). Secondary outcomes included the overall rate of morbidity. Outcomes were assessed up to 90 days postoperatively. Overall, 120 patients per group were required to achieve 80% power and detect at least 30% reduction in the CCI in the SPN group, which was expected to be 23 (median) (interquartile range 21-31). The expected complication rate was 60%, and the type I error rate was set at 5%. Registration at ClinicalTrials.gov (#NCT04438447).
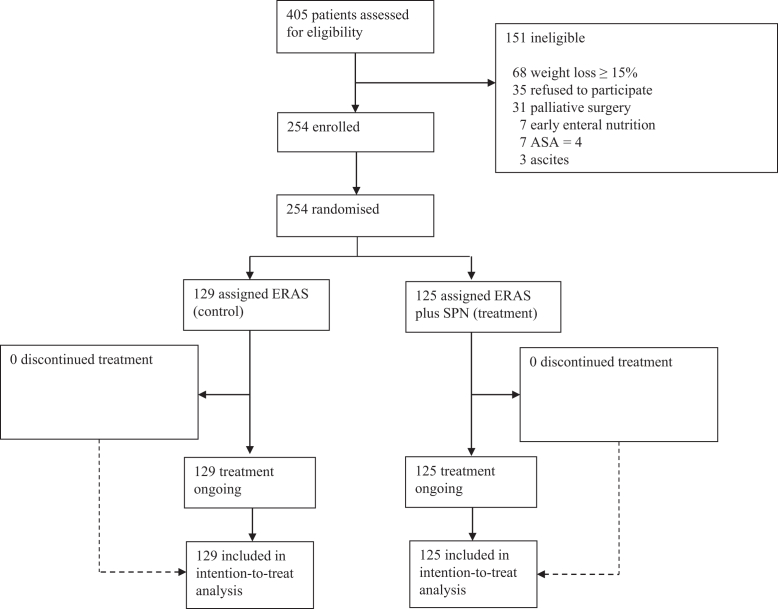
Findings: From June 1, 2022, to December 20, 2023, 405 patients were screened for eligibility and 254 patients were randomly allocated to control (no-SPN; n = 129) or treatment (SPN; n = 125) group. All patients were included in the primary and secondary outcome analysis according to the intent-to-treat principle. The median CCI was 20.9 in both arms (median difference 0 [95% CI: -1.07 to 1.7]). The proportion of patients with at least one complication (CCI >0) was similar in both groups [(29.6% vs 29.2%; risk difference 0.4 (95% CI -11.1 to 7.0)]. The overall 90-day morbidity was 67.4% and 63.2% in the no-SPN arm and SPN arm groups, respectively [risk difference -4.2 (95% CI -16.7 to 8.2)]. In high nutritional risk patients (nutritional risk score ≥3), SPN was not protective against the primary outcome when compared with low-risk patients [OR 1.16 (95% CI 0.71-1.91)].
Interpretation: In an ERAS program emphasizing early postoperative oral feeding, SPN does not affect outcome measures, even in patients at high nutritional risk. However, these results do not apply to severely malnourished patients or with critical comorbidities.
Funding: The Italian Society for Artificial Nutrition and Metabolism (SINPE) and Baxter Italia S.p.A (Rome, Italy).
背景:胰十二指肠切除术(PD)后补充肠外营养(SPN)在增强恢复计划中的作用尚未探讨。本研究旨在确定SPN在减少术后并发症方面是否优于早期单独口服喂养。方法:这项实用的、多中心的、随机对照的试验,在意大利的五个中心进行,招募了年龄在18-89岁之间接受开放式PD治疗的癌症患者。我们排除了美国麻醉学会评定身体状况为bbbb3且术前体重减轻≥15%的患者。术后1 - 5天,患者被随机(1:1)分配至SPN组或无SPN组。所有患者均可在术后完全增强恢复(ERAS)计划的背景下,自由开始口服喂养。主要终点是发病率负担,用综合并发症指数(CCI)来衡量。次要结局包括总体发病率。随访至术后90天。总体而言,每组需要120例患者才能达到80%的疗效,并检测到SPN组CCI降低至少30%,预期为23(中位数)(四分位数范围21-31)。预期并发症率为60%,I型错误率设为5%。在ClinicalTrials.gov注册(#NCT04438447)。结果:从2022年6月1日至2023年12月20日,筛选了405例患者,将254例患者随机分为对照组(无SPN, n = 129)和治疗组(SPN, n = 125)。根据意向治疗原则,将所有患者纳入主要和次要结局分析。两组的中位CCI均为20.9(中位差异为0 [95% CI: -1.07至1.7])。两组至少有一种并发症(CCI bb0 0)的患者比例相似[(29.6% vs 29.2%;风险差0.4 (95% CI -11.1 ~ 7.0)]。无SPN组和SPN组90天总发病率分别为67.4%和63.2%[风险差-4.2 (95% CI -16.7 ~ 8.2)]。在高营养风险患者(营养风险评分≥3)中,与低风险患者相比,SPN对主要结局没有保护作用[OR 1.16 (95% CI 0.71-1.91)]。解释:在强调术后早期口服喂养的ERAS项目中,SPN不影响结果测量,即使在高营养风险患者中也是如此。然而,这些结果并不适用于严重营养不良或严重合并症的患者。资助:意大利人工营养与代谢学会(SINPE)和意大利百特公司(罗马,意大利)。
期刊介绍:
eClinicalMedicine is a gold open-access clinical journal designed to support frontline health professionals in addressing the complex and rapid health transitions affecting societies globally. The journal aims to assist practitioners in overcoming healthcare challenges across diverse communities, spanning diagnosis, treatment, prevention, and health promotion. Integrating disciplines from various specialties and life stages, it seeks to enhance health systems as fundamental institutions within societies. With a forward-thinking approach, eClinicalMedicine aims to redefine the future of healthcare.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


