Outcomes of ureteroscopy and laser lithotripsy with and without ureteral access sheaths for the treatment of renal calculi: A systematic review and meta-analysis.
{"title":"Outcomes of ureteroscopy and laser lithotripsy with and without ureteral access sheaths for the treatment of renal calculi: A systematic review and meta-analysis.","authors":"James Connor, Steven Anderson, Niall F Davis","doi":"10.5173/ceju.2024.0196","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The use of ureteral access sheaths (UASs) is an issue of contention among urologists, with their efficacy unclear in retrograde intrarenal surgery (RIRS). Therefore, we performed a systematic review and meta-analysis to assess RIRS with laser lithotripsy for the treatment of urolithiasis with and without the use of UASs.</p><p><strong>Material and methods: </strong>A systematic literature search was conducted in July 2023 using MEDLINE, EMBASE and the Cochrane library. The quality of the included studies was assessed using the Newcastle-Ottowa scale and Cochrane collaboration risk of bias tool. The primary outcome measures were stone-free rate (SFR), and post-operative complications. Secondary outcomes were operative time (OT), hospital length of stay (LOS) and ureteral injury rate. Effect sizes were calculated by pooled risk ratios (RRs) and mean differences (MDs) with confidence intervals (CIs).</p><p><strong>Results: </strong>In total, 16 studies met the inclusion criteria. There were 3,123 participants who had RIRS with a UAS and 1,478 without. Pooled analysis revealed no significant difference between groups in SFR (RR = 1.03, 95% CI: 0.99-1.07), complication rate (RR = 1.31, 95% CI: 1.00-1.73), ureteral injuries (RR = 1.13, 95% CI: 0.77-1.65) or LOS (MD = -0.01, 95% CI: from -0.08 to 0.11). OT was significantly longer in the UAS group (MD = 0.35, 95% CI: 0.01-0.7).</p><p><strong>Conclusions: </strong>The results of this meta-analysis demonstrate that the use of UASs during RIRS does not improve post-operative outcomes and is associated with a longer OT. While there are still times where the use of UASs may be beneficial, their routine use for patients undergoing RIRS is not currently indicated.</p>","PeriodicalId":9744,"journal":{"name":"Central European Journal of Urology","volume":"78 2","pages":"228-236"},"PeriodicalIF":1.9000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12379812/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Central European Journal of Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5173/ceju.2024.0196","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/5/25 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The use of ureteral access sheaths (UASs) is an issue of contention among urologists, with their efficacy unclear in retrograde intrarenal surgery (RIRS). Therefore, we performed a systematic review and meta-analysis to assess RIRS with laser lithotripsy for the treatment of urolithiasis with and without the use of UASs.
Material and methods: A systematic literature search was conducted in July 2023 using MEDLINE, EMBASE and the Cochrane library. The quality of the included studies was assessed using the Newcastle-Ottowa scale and Cochrane collaboration risk of bias tool. The primary outcome measures were stone-free rate (SFR), and post-operative complications. Secondary outcomes were operative time (OT), hospital length of stay (LOS) and ureteral injury rate. Effect sizes were calculated by pooled risk ratios (RRs) and mean differences (MDs) with confidence intervals (CIs).
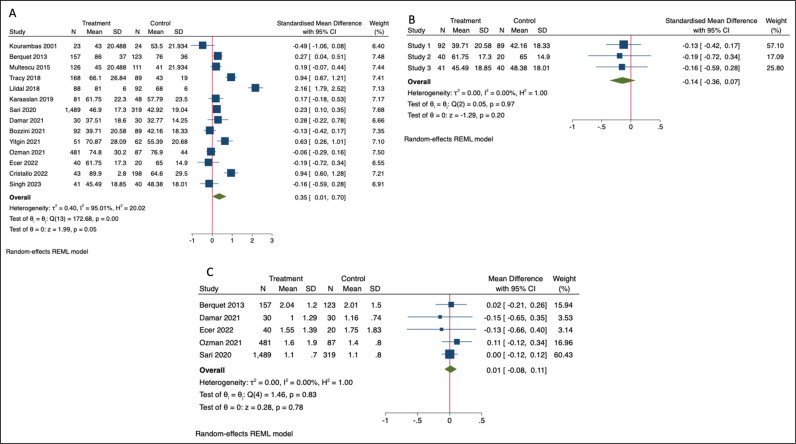
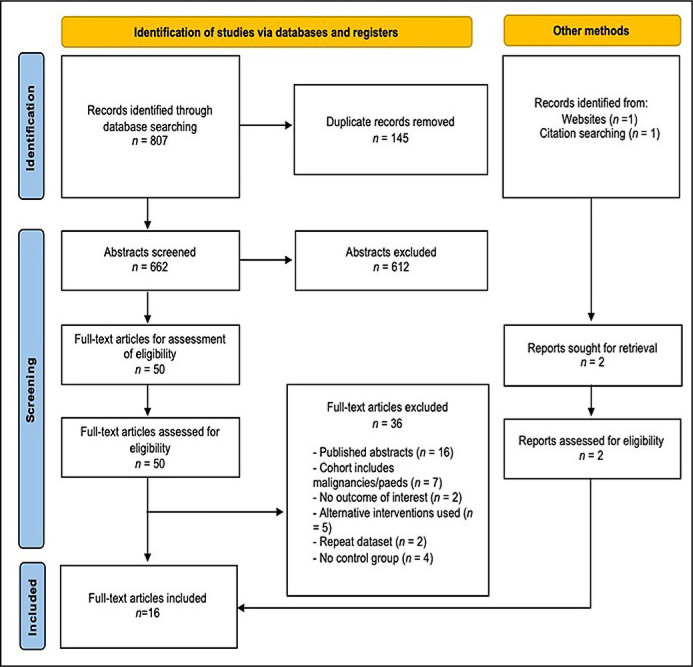
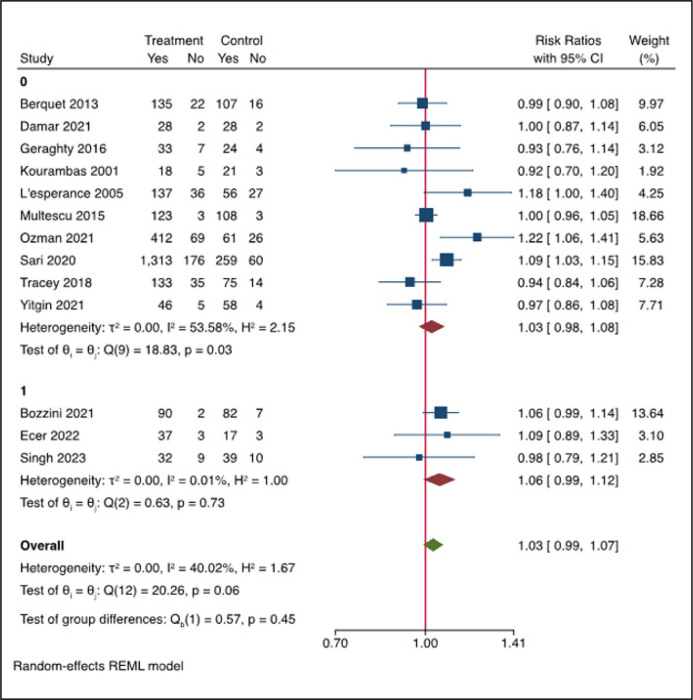
Results: In total, 16 studies met the inclusion criteria. There were 3,123 participants who had RIRS with a UAS and 1,478 without. Pooled analysis revealed no significant difference between groups in SFR (RR = 1.03, 95% CI: 0.99-1.07), complication rate (RR = 1.31, 95% CI: 1.00-1.73), ureteral injuries (RR = 1.13, 95% CI: 0.77-1.65) or LOS (MD = -0.01, 95% CI: from -0.08 to 0.11). OT was significantly longer in the UAS group (MD = 0.35, 95% CI: 0.01-0.7).
Conclusions: The results of this meta-analysis demonstrate that the use of UASs during RIRS does not improve post-operative outcomes and is associated with a longer OT. While there are still times where the use of UASs may be beneficial, their routine use for patients undergoing RIRS is not currently indicated.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


