{"title":"Balancing technology and resources: Is robotic pyeloplasty always necessary?","authors":"Kunal Malhotra, Vikas Kumar Panwar, Gautam Shubhankar, Ankur Mittal, Mohammed Taher Mujahid","doi":"10.5173/ceju.2024.0203","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Ureteropelvic junction obstruction (UPJO) hinders urine flow from the renal pelvis to the ureter, causing renal dysfunction. Treatment focuses on relieving obstruction to restore urinary drainage and preserve renal function. Robotic-assisted laparoscopic pyeloplasty (RALP) offers enhanced precision compared to laparoscopic pyeloplasty (LP), but limited comparative data exist for adult patients. This study compares RALP and LP outcomes in an adult cohort from a tertiary care centre.</p><p><strong>Material and methods: </strong>A retrospective cohort analysis was conducted on adult patients who underwent RALP or LP between March 2018 and May 2024. Primary outcome measures included operative time, with secondary outcomes such as estimated blood loss (EBL), hospital length of stay (LOS), complication rates, and success (defined by symptom relief and diuretic renogram improvement). Statistical analysis included Mann-Whitney, χ<sup>2</sup>, and Fisher's exact tests, with a significance threshold of p <0.05.</p><p><strong>Results: </strong>The study included 128 patients (87 RALP, 41 LP). Operative time was significantly longer for RALP (200.92 ±59.26 minutes) vs LP (161.92 ±55.21 minutes, p <0.001), largely due to robotic docking. Both groups had similar EBL (47.87 ml for RALP vs 45 ml for LP, p = 0.45) and success rates (97.7% for RALP vs 97.4% for LP). However, RALP patients experienced a longer LOS (3.91 days vs 3.41 days, p = 0.001).</p><p><strong>Conclusions: </strong>RALP demonstrates technical advantages but does not reduce operative time and incurs increased resource utilisation compared to LP. Both techniques achieve high success rates, though further research is needed to assess RALP's cost-effectiveness.</p>","PeriodicalId":9744,"journal":{"name":"Central European Journal of Urology","volume":"78 2","pages":"244-249"},"PeriodicalIF":1.9000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12379814/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Central European Journal of Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5173/ceju.2024.0203","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/4/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Ureteropelvic junction obstruction (UPJO) hinders urine flow from the renal pelvis to the ureter, causing renal dysfunction. Treatment focuses on relieving obstruction to restore urinary drainage and preserve renal function. Robotic-assisted laparoscopic pyeloplasty (RALP) offers enhanced precision compared to laparoscopic pyeloplasty (LP), but limited comparative data exist for adult patients. This study compares RALP and LP outcomes in an adult cohort from a tertiary care centre.
Material and methods: A retrospective cohort analysis was conducted on adult patients who underwent RALP or LP between March 2018 and May 2024. Primary outcome measures included operative time, with secondary outcomes such as estimated blood loss (EBL), hospital length of stay (LOS), complication rates, and success (defined by symptom relief and diuretic renogram improvement). Statistical analysis included Mann-Whitney, χ2, and Fisher's exact tests, with a significance threshold of p <0.05.
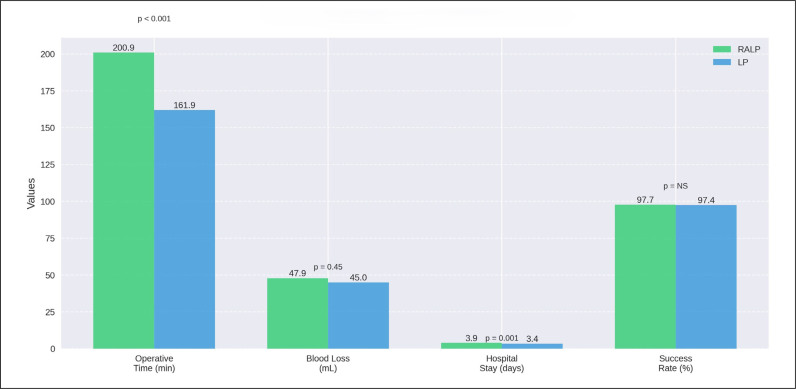
Results: The study included 128 patients (87 RALP, 41 LP). Operative time was significantly longer for RALP (200.92 ±59.26 minutes) vs LP (161.92 ±55.21 minutes, p <0.001), largely due to robotic docking. Both groups had similar EBL (47.87 ml for RALP vs 45 ml for LP, p = 0.45) and success rates (97.7% for RALP vs 97.4% for LP). However, RALP patients experienced a longer LOS (3.91 days vs 3.41 days, p = 0.001).
Conclusions: RALP demonstrates technical advantages but does not reduce operative time and incurs increased resource utilisation compared to LP. Both techniques achieve high success rates, though further research is needed to assess RALP's cost-effectiveness.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


