Development and validation of a postpartum cardiovascular disease risk prediction model in women incorporating reproductive and pregnancy-related predictors.
Steven Wambua, Francesca L Crowe, Shakila Thangaratinam, Dermot O'Reilly, Colin McCowan, Sinead Brophy, Christopher Yau, Krishnarajah Nirantharakumar, Richard D Riley, Kym I E Snell
{"title":"Development and validation of a postpartum cardiovascular disease risk prediction model in women incorporating reproductive and pregnancy-related predictors.","authors":"Steven Wambua, Francesca L Crowe, Shakila Thangaratinam, Dermot O'Reilly, Colin McCowan, Sinead Brophy, Christopher Yau, Krishnarajah Nirantharakumar, Richard D Riley, Kym I E Snell","doi":"10.1186/s12916-025-04229-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Each year, over 700,000 pregnancies occur in the UK, with up to 10% affected by complications such as hypertensive disorders of pregnancy and gestational diabetes mellitus. Pregnancy-related complications and reproductive factors are associated with an increased risk of cardiovascular disease (CVD) later in life. Our aim was to determine whether adding pregnancy factors to a prediction model with established CVD risk factors improves 10-year risk prediction of CVD in postpartum women, using QRISK®-3 as a benchmark model.</p><p><strong>Methods: </strong>We used a population-based retrospective cohort of women aged 15 to 49 who had been pregnant from the Clinical Practice Research Datalink (CPRD) primary care database. Women who were CVD-free were followed from 6 months postpartum. We evaluated the performance of QRISK®-3 and updated the risk prediction model using established risk factors for CVD from QRISK®-3 and additional risk factors specific to pregnancy. Models were developed using Cox-proportional hazards regression for CVD within 10 years. Models were evaluated and compared using measures of overall model fit, calibration, discrimination and clinical utility.</p><p><strong>Results: </strong>Among 567,667 eligible women, 2175 (0.38%) experienced a CVD event within 10 years. The median follow-up was 4 years. Of the additional pregnancy factors, gestational hypertension, preeclampsia, miscarriage, stillbirth, postnatal depression, gravidity, endometriosis and polycystic ovary syndrome remained associated with CVD after adjusting for other established risk factors of CVD. Adding pregnancy factors to those from QRISK®-3 led to marginal improvements in model performance (QRISK®-3 C-statistic: 0.703 (95% CI 0.687 to 0.718), updated model C-statistic: 0.726 (95% CI 0.711 to 0.740) Although calibration did not improve overall, subgroup analysis showed better calibration in women with a history of pre-eclampsia, postnatal depression and preterm birth using the updated model. The clinical utility was improved for updated models.</p><p><strong>Conclusions: </strong>The updated risk prediction models resulted in marginal improvement in discrimination and calibration compared to QRISK®-3 in postpartum women. This could be due to the known association of pregnancy-related complications with established risk factors of CVD. Although the overall predictive performance and calibration of the updated models was similar, the updated model resulted in better clinical utility.</p>","PeriodicalId":9188,"journal":{"name":"BMC Medicine","volume":"23 1","pages":"508"},"PeriodicalIF":8.3000,"publicationDate":"2025-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12398157/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12916-025-04229-1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Each year, over 700,000 pregnancies occur in the UK, with up to 10% affected by complications such as hypertensive disorders of pregnancy and gestational diabetes mellitus. Pregnancy-related complications and reproductive factors are associated with an increased risk of cardiovascular disease (CVD) later in life. Our aim was to determine whether adding pregnancy factors to a prediction model with established CVD risk factors improves 10-year risk prediction of CVD in postpartum women, using QRISK®-3 as a benchmark model.
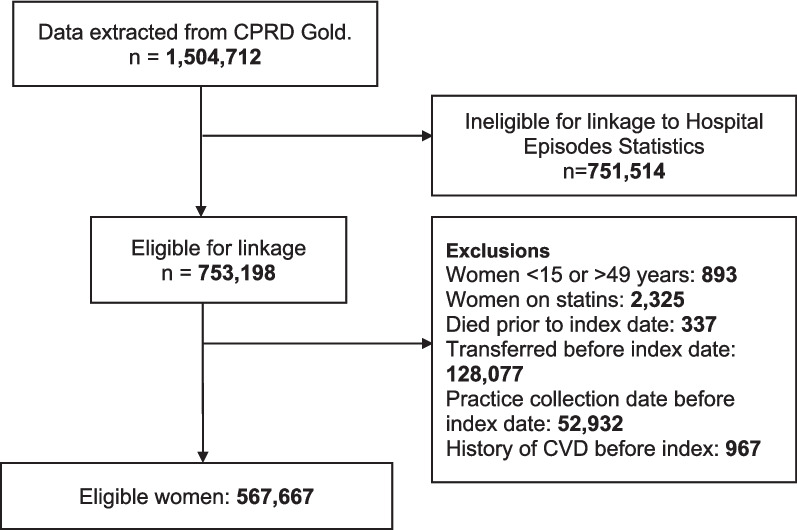
Methods: We used a population-based retrospective cohort of women aged 15 to 49 who had been pregnant from the Clinical Practice Research Datalink (CPRD) primary care database. Women who were CVD-free were followed from 6 months postpartum. We evaluated the performance of QRISK®-3 and updated the risk prediction model using established risk factors for CVD from QRISK®-3 and additional risk factors specific to pregnancy. Models were developed using Cox-proportional hazards regression for CVD within 10 years. Models were evaluated and compared using measures of overall model fit, calibration, discrimination and clinical utility.
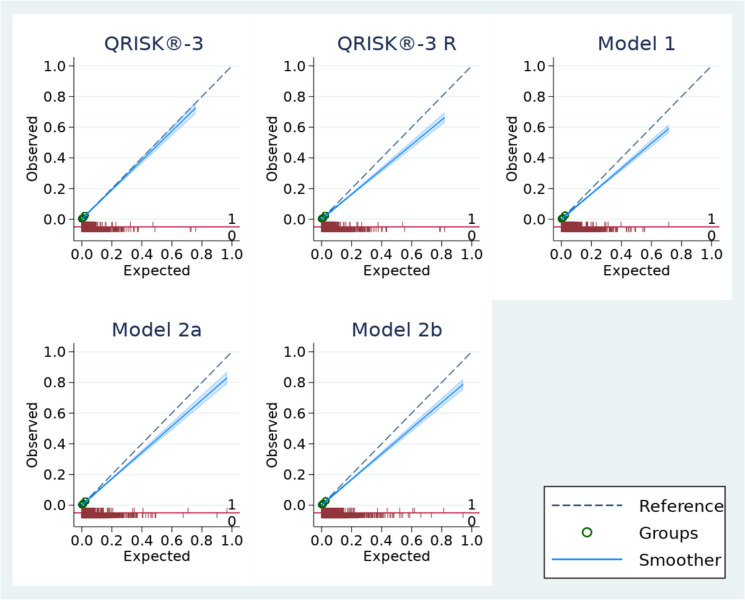
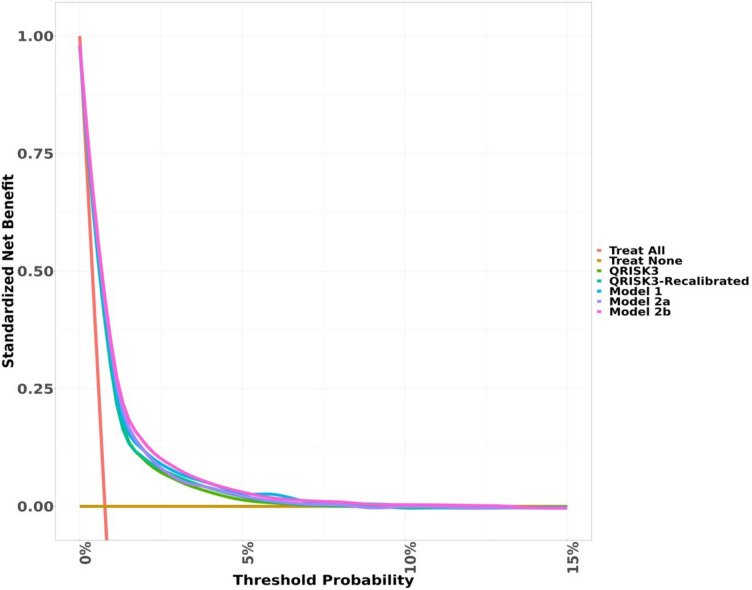
Results: Among 567,667 eligible women, 2175 (0.38%) experienced a CVD event within 10 years. The median follow-up was 4 years. Of the additional pregnancy factors, gestational hypertension, preeclampsia, miscarriage, stillbirth, postnatal depression, gravidity, endometriosis and polycystic ovary syndrome remained associated with CVD after adjusting for other established risk factors of CVD. Adding pregnancy factors to those from QRISK®-3 led to marginal improvements in model performance (QRISK®-3 C-statistic: 0.703 (95% CI 0.687 to 0.718), updated model C-statistic: 0.726 (95% CI 0.711 to 0.740) Although calibration did not improve overall, subgroup analysis showed better calibration in women with a history of pre-eclampsia, postnatal depression and preterm birth using the updated model. The clinical utility was improved for updated models.
Conclusions: The updated risk prediction models resulted in marginal improvement in discrimination and calibration compared to QRISK®-3 in postpartum women. This could be due to the known association of pregnancy-related complications with established risk factors of CVD. Although the overall predictive performance and calibration of the updated models was similar, the updated model resulted in better clinical utility.
背景:英国每年有超过70万例怀孕,其中高达10%的孕妇患有妊娠期高血压和妊娠期糖尿病等并发症。妊娠相关并发症和生殖因素与生命后期心血管疾病(CVD)风险增加有关。我们的目的是使用QRISK®-3作为基准模型,确定在已有CVD危险因素的预测模型中加入妊娠因素是否能改善产后妇女CVD 10年风险预测。方法:我们采用基于人群的回顾性队列研究,研究对象是来自临床实践研究数据链(CPRD)初级保健数据库的15至49岁怀孕妇女。没有心血管疾病的妇女从产后6个月开始接受随访。我们评估了QRISK®-3的性能,并使用QRISK®-3中CVD的既定危险因素和妊娠特有的其他危险因素更新了风险预测模型。采用cox -比例风险回归方法建立10年内心血管疾病的模型。使用整体模型拟合、校准、鉴别和临床效用等措施对模型进行评估和比较。结果:在567,667名符合条件的女性中,2175名(0.38%)在10年内经历过心血管疾病事件。中位随访时间为4年。在其他妊娠因素中,妊娠期高血压、先兆子痫、流产、死产、产后抑郁、妊娠、子宫内膜异位症和多囊卵巢综合征在校正其他已确定的CVD危险因素后仍与CVD相关。在QRISK®-3中加入妊娠因素导致模型性能的边际改善(QRISK®-3 c -统计量:0.703 (95% CI 0.687至0.718),更新后的模型c -统计量:0.726 (95% CI 0.711至0.740)。尽管校准总体上没有改善,但亚组分析显示,使用更新后的模型,有先兆子痫、产后抑郁和早产史的妇女的校准效果更好。更新后的模型改善了临床应用。结论:与QRISK®-3相比,更新后的风险预测模型在产后妇女的辨别和校准方面有了边际改善。这可能是由于已知的妊娠相关并发症与心血管疾病的既定危险因素有关。虽然更新后的模型的总体预测性能和校准相似,但更新后的模型具有更好的临床效用。
期刊介绍:
BMC Medicine is an open access, transparent peer-reviewed general medical journal. It is the flagship journal of the BMC series and publishes outstanding and influential research in various areas including clinical practice, translational medicine, medical and health advances, public health, global health, policy, and general topics of interest to the biomedical and sociomedical professional communities. In addition to research articles, the journal also publishes stimulating debates, reviews, unique forum articles, and concise tutorials. All articles published in BMC Medicine are included in various databases such as Biological Abstracts, BIOSIS, CAS, Citebase, Current contents, DOAJ, Embase, MEDLINE, PubMed, Science Citation Index Expanded, OAIster, SCImago, Scopus, SOCOLAR, and Zetoc.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


