{"title":"Intraoperative extracorporeal life support in tracheal surgery: a 20-year single-center experience.","authors":"Lin Sun, Liping Xin, Yuwei Qiu, Lingfeng Xu, Xin Chang, Xiaoyu Zhou, Zhen Guo","doi":"10.1186/s12871-025-03285-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Despite advancements in perioperative management, patients undergoing complex tracheal surgery still face increased risks of morbidity and mortality. Extracorporeal life support (ECLS) can be utilized to maintain hemodynamic and respiratory stability during surgical procedures, but there is currently no evidence-based practice protocol in place. This study seeks to evaluate the safety and benefits of various ECLS modes in critical tracheal surgery and establish a practical protocol for the application of ECLS.</p><p><strong>Methods: </strong>Single center, retrospective, cohort study. This retrospective study collected data on patients who underwent tracheal procedures on ECLS between January 2000 and December 2020. Patients were divided into three groups according to configuration: cardiopulmonary bypass (CPB), modified CPB and extracorporeal membrane oxygenation (ECMO). Baseline characteristics, in-hospital complications, ECLS details, adverse events, and overall survival were assessed and compared between three groups.</p><p><strong>Results: </strong>Over twenty years period, from 462 primary tracheal disease patients, 67 patients were identified from our institutional medical registry as having received CPB, modified-CPB or ECMO during the procedure (26.9%, 22.4% and 50.7% respectively). Heparin free (n = 30, 44.8%) or low dose heparin (n = 17, 26.6%) therapy was frequently utilized in ECMO and modified-CPB group. The Median pump duration of CPB, modified-CPB, VV, and VA ECMO was 43, 64, 139, and 127 min. Anastomotic complications were significantly lower in the VV-ECMO group (7.1%), while the duration of mechanical ventilation was significantly longer in the VA-ECMO group (66, [2-178]). Surgical bleeding was significantly higher in the CPB group (460 ± 73 ml). More patients in the CPB group (9/18) required blood transfusions; however, there was no significant difference in the volume of packed red blood cells between the groups.</p><p><strong>Conclusion: </strong>Despite intraoperative ECLS being rarely used in tracheal and carinal disease, programmed extracorporeal life support with VV-ECMO demonstrated high effectiveness with an acceptable mortality and morbidity rate in high-risk tracheal surgery.</p>","PeriodicalId":9190,"journal":{"name":"BMC Anesthesiology","volume":"25 1","pages":"425"},"PeriodicalIF":2.6000,"publicationDate":"2025-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12379321/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Anesthesiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12871-025-03285-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Despite advancements in perioperative management, patients undergoing complex tracheal surgery still face increased risks of morbidity and mortality. Extracorporeal life support (ECLS) can be utilized to maintain hemodynamic and respiratory stability during surgical procedures, but there is currently no evidence-based practice protocol in place. This study seeks to evaluate the safety and benefits of various ECLS modes in critical tracheal surgery and establish a practical protocol for the application of ECLS.
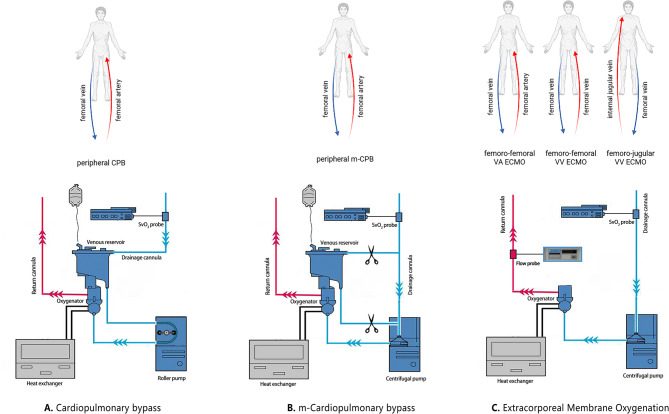
Methods: Single center, retrospective, cohort study. This retrospective study collected data on patients who underwent tracheal procedures on ECLS between January 2000 and December 2020. Patients were divided into three groups according to configuration: cardiopulmonary bypass (CPB), modified CPB and extracorporeal membrane oxygenation (ECMO). Baseline characteristics, in-hospital complications, ECLS details, adverse events, and overall survival were assessed and compared between three groups.
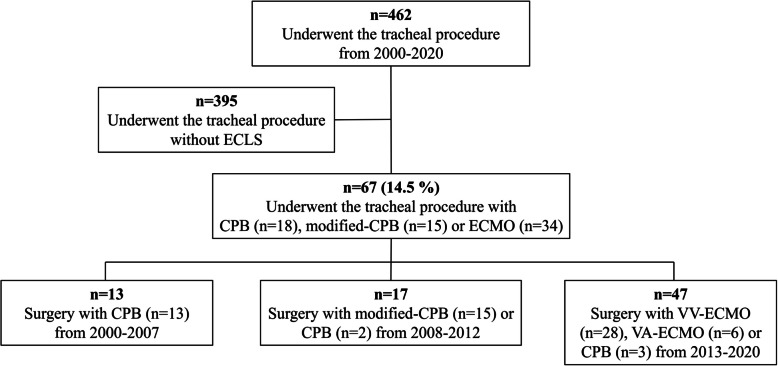
Results: Over twenty years period, from 462 primary tracheal disease patients, 67 patients were identified from our institutional medical registry as having received CPB, modified-CPB or ECMO during the procedure (26.9%, 22.4% and 50.7% respectively). Heparin free (n = 30, 44.8%) or low dose heparin (n = 17, 26.6%) therapy was frequently utilized in ECMO and modified-CPB group. The Median pump duration of CPB, modified-CPB, VV, and VA ECMO was 43, 64, 139, and 127 min. Anastomotic complications were significantly lower in the VV-ECMO group (7.1%), while the duration of mechanical ventilation was significantly longer in the VA-ECMO group (66, [2-178]). Surgical bleeding was significantly higher in the CPB group (460 ± 73 ml). More patients in the CPB group (9/18) required blood transfusions; however, there was no significant difference in the volume of packed red blood cells between the groups.
Conclusion: Despite intraoperative ECLS being rarely used in tracheal and carinal disease, programmed extracorporeal life support with VV-ECMO demonstrated high effectiveness with an acceptable mortality and morbidity rate in high-risk tracheal surgery.
期刊介绍:
BMC Anesthesiology is an open access, peer-reviewed journal that considers articles on all aspects of anesthesiology, critical care, perioperative care and pain management, including clinical and experimental research into anesthetic mechanisms, administration and efficacy, technology and monitoring, and associated economic issues.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


