Tedy Sawma MD , Hartzell V. Schaff MD , Anita Zheng MD , Gokce Belge Bilgin MD , Thorvardur R. Halfdanarson MD , S.Allen Luis MD, PhD , Patricia A. Pellikka MD , Heidi M. Connolly MD , Juan A. Crestanello MD
{"title":"Outcomes of surgical management of carcinoid heart disease in patients with primary gonadal neuroendocrine tumors","authors":"Tedy Sawma MD , Hartzell V. Schaff MD , Anita Zheng MD , Gokce Belge Bilgin MD , Thorvardur R. Halfdanarson MD , S.Allen Luis MD, PhD , Patricia A. Pellikka MD , Heidi M. Connolly MD , Juan A. Crestanello MD","doi":"10.1016/j.xjon.2025.05.010","DOIUrl":null,"url":null,"abstract":"<div><h3>Objectives</h3><div>To describe the clinical presentation of patients with gonadal neuroendocrine tumors and carcinoid heart disease (CaHD) and to evaluate long-term outcomes following valvular surgery.</div></div><div><h3>Methods</h3><div>Retrospective review of patients with primary gonadal neuroendocrine tumor who were surgically treated for CaHD at our institution between 1990 and 2021.</div></div><div><h3>Results</h3><div>Eight patients (median age, 70 years) were included in the study, 7 with ovarian tumors and 1 with testicular tumor. None of the patients had liver metastasis at the time of cardiac surgery. Three patients presented with both CaHD symptoms and carcinoid syndrome symptoms (diarrhea and flushing). Three others presented with symptoms of CaHD but without diarrhea or flushing. One patient with ovarian tumor presented with severe diarrhea and flushing without CaHD symptoms and had tumor resection but then developed severe CaHD symptoms few months later. The last patient presented initially with an asymptomatic testicular mass, which was resected, but then developed severe CaHD symptoms years later. All patients had severe tricuspid regurgitation at time of surgery, and 7 had severe pulmonary regurgitation. All were treated with replacement of affected valves. Both 5- and 10-year survival rates were 86% and were higher than a control group of patients with CaHD and nongonadal primary neuroendocrine tumor (35% and 23%, respectively).</div></div><div><h3>Conclusions</h3><div>Patients with primary gonadal neuroendocrine tumors can develop CaHD in the absence of liver metastasis. Some patients have delayed presentation of cardiac symptoms, emphasizing the importance of thorough assessment and regular echocardiographic follow-up. Cardiac intervention is safe and yields excellent long-term survival.</div></div>","PeriodicalId":74032,"journal":{"name":"JTCVS open","volume":"26 ","pages":"Pages 115-121"},"PeriodicalIF":1.9000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JTCVS open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666273625002062","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives
To describe the clinical presentation of patients with gonadal neuroendocrine tumors and carcinoid heart disease (CaHD) and to evaluate long-term outcomes following valvular surgery.
Methods
Retrospective review of patients with primary gonadal neuroendocrine tumor who were surgically treated for CaHD at our institution between 1990 and 2021.
Results
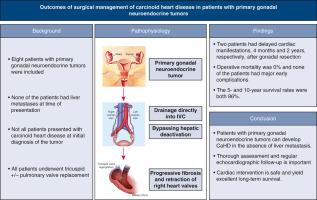
Eight patients (median age, 70 years) were included in the study, 7 with ovarian tumors and 1 with testicular tumor. None of the patients had liver metastasis at the time of cardiac surgery. Three patients presented with both CaHD symptoms and carcinoid syndrome symptoms (diarrhea and flushing). Three others presented with symptoms of CaHD but without diarrhea or flushing. One patient with ovarian tumor presented with severe diarrhea and flushing without CaHD symptoms and had tumor resection but then developed severe CaHD symptoms few months later. The last patient presented initially with an asymptomatic testicular mass, which was resected, but then developed severe CaHD symptoms years later. All patients had severe tricuspid regurgitation at time of surgery, and 7 had severe pulmonary regurgitation. All were treated with replacement of affected valves. Both 5- and 10-year survival rates were 86% and were higher than a control group of patients with CaHD and nongonadal primary neuroendocrine tumor (35% and 23%, respectively).
Conclusions
Patients with primary gonadal neuroendocrine tumors can develop CaHD in the absence of liver metastasis. Some patients have delayed presentation of cardiac symptoms, emphasizing the importance of thorough assessment and regular echocardiographic follow-up. Cardiac intervention is safe and yields excellent long-term survival.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


