Takuya Ogami MD , Ethan Chetkof BS , Johannes O. Bonatti MD , Christopher Pantelis BS , Stephen D. Waterford MD , Francis D. Ferdinand MD , Irsa S. Hasan MD , Derek Serna-Gallegos MD , David J. Kaczorowski MD , Danny Chu MD , Floyd W. Thoma BS , Ibrahim Sultan MD
{"title":"Posterior leaflet reconstruction in mitral valve repair: Does resect versus respect strategy matter?","authors":"Takuya Ogami MD , Ethan Chetkof BS , Johannes O. Bonatti MD , Christopher Pantelis BS , Stephen D. Waterford MD , Francis D. Ferdinand MD , Irsa S. Hasan MD , Derek Serna-Gallegos MD , David J. Kaczorowski MD , Danny Chu MD , Floyd W. Thoma BS , Ibrahim Sultan MD","doi":"10.1016/j.xjon.2025.06.009","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><div>Previous randomized controlled trials demonstrated comparable outcomes between posterior leaflet resections and neochord implantation in mitral valve (MV) repair. However, these studies were limited up to 1-year follow-up, and more recent evidence suggested that leaflet resections may offer superior long-term outcomes.</div></div><div><h3>Methods</h3><div>All patients who underwent MV repair with either resection or neochord implantation for posterior leaflet pathology between October 2011 and July 2024 were included. Propensity-score matching was used.</div></div><div><h3>Results</h3><div>A total of 457 patients underwent posterior leaflet reconstruction, with 334 (73.1%) requiring leaflet resection (resection group) and 123 (26.9%) receiving neochordae (neochord group). The median [interquartile range] follow-up for survival and reintervention was 5.93 [2.00, 9.09] and 5.48 [1.84, 9.02] years, respectively. Overall, the mean age was 63.9 years, and the mean ejection fraction was 58.9%. Robotic-assisted surgery was performed in 28.9% (n = 132). The 30-day mortality was 2.4% (n = 11). Propensity-score matching provided 119 patients in each group. Kaplan-Meier curves demonstrated similar survival at 5 years between these groups (93.1 ± 2.8% in the resection group and 89.6 ± 3.1% in the neochord group, <em>P</em> = .5). However, the neochord group had a greater cumulative incidence of reoperative MV surgery (8.0% vs 0.9% at 5 years in the resection group, <em>P</em> = .01).</div></div><div><h3>Conclusions</h3><div>Neochordae were implanted in 27.3% of patients undergoing MV repair. Neochord implantation was associated with a greater risk of MV reintervention in the long term. Careful patient selection and technical considerations are important when choosing the repair method.</div></div>","PeriodicalId":74032,"journal":{"name":"JTCVS open","volume":"26 ","pages":"Pages 94-103"},"PeriodicalIF":1.9000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JTCVS open","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666273625002153","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
Previous randomized controlled trials demonstrated comparable outcomes between posterior leaflet resections and neochord implantation in mitral valve (MV) repair. However, these studies were limited up to 1-year follow-up, and more recent evidence suggested that leaflet resections may offer superior long-term outcomes.
Methods
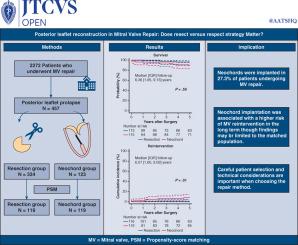
All patients who underwent MV repair with either resection or neochord implantation for posterior leaflet pathology between October 2011 and July 2024 were included. Propensity-score matching was used.
Results
A total of 457 patients underwent posterior leaflet reconstruction, with 334 (73.1%) requiring leaflet resection (resection group) and 123 (26.9%) receiving neochordae (neochord group). The median [interquartile range] follow-up for survival and reintervention was 5.93 [2.00, 9.09] and 5.48 [1.84, 9.02] years, respectively. Overall, the mean age was 63.9 years, and the mean ejection fraction was 58.9%. Robotic-assisted surgery was performed in 28.9% (n = 132). The 30-day mortality was 2.4% (n = 11). Propensity-score matching provided 119 patients in each group. Kaplan-Meier curves demonstrated similar survival at 5 years between these groups (93.1 ± 2.8% in the resection group and 89.6 ± 3.1% in the neochord group, P = .5). However, the neochord group had a greater cumulative incidence of reoperative MV surgery (8.0% vs 0.9% at 5 years in the resection group, P = .01).
Conclusions
Neochordae were implanted in 27.3% of patients undergoing MV repair. Neochord implantation was associated with a greater risk of MV reintervention in the long term. Careful patient selection and technical considerations are important when choosing the repair method.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


