Dosimetric feasibility of stereotactic arrhythmia radioablation for ventricular tachycardia in patients with a subcutaneous implantable cardioverter defibrillator
IF 3.3
Q2 ONCOLOGY
引用次数: 0
Abstract
Background and purpose
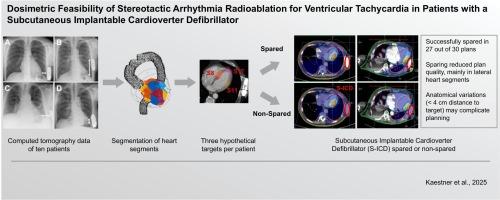
Subcutaneous implantable cardioverter defibrillators (S-ICDs) are increasingly used to prevent sudden cardiac death. Due to their placement near the left lateral and apical myocardium, S-ICDs can present technical challenges for stereotactic arrhythmia radioablation (STAR) of ventricular tachycardia. This study aimed to evaluate the feasibility of STAR in patients with S-ICDs.
Materials and methods
Previously acquired cardiac computed tomography data from ten S-ICD patients were retrospectively analyzed. Organs at risk, S-ICD components, and hypothetical planning target volumes (PTV) for segments 8 (septal), 11 (lateral), and 17 (apical) were contoured. For each patient and segment, two treatment plans were calculated with a prescribed PTV dose of 25 Gy: one plan sparing the S-ICD from the primary radiotherapy beam (‘spared’) and one without this constraint (‘non-spared’).
Results
The S-ICD was successfully spared from the primary beam in 27 out of 30 plans, with D0.035cm3 < 1 Gy. In three spared plans (PTV segment 11) with a distance between PTV and S-ICD <4 cm, D0.035cm3 exceeded 1 Gy. Spared plans for PTV segment 11 showed significant higher dose/volume metrics and reduced plan quality compared to non-spared plans (p < 0.05), although 9/10 plans remained clinically acceptable. For PTV segment 8 and segment 17, no clinical or statistical differences were observed.
Conclusions
The presence of an S-ICD is not a contraindication for STAR, although plan quality may decrease with PTVs in lateral segments. Rare cases with a distance between PTV and S-ICD <4 cm may complicate radiation treatment planning.
立体定向心律失常放射消融治疗皮下植入式心律转复除颤器患者室性心动过速的剂量学可行性
背景与目的:皮下植入式心律转复除颤器(S-ICDs)越来越多地用于预防心源性猝死。由于s - icd放置在左外侧和顶端心肌附近,因此对室性心动过速的立体定向心律失常放射消融(STAR)提出了技术挑战。本研究旨在评估STAR在s - icd患者中的可行性。材料和方法回顾性分析10例S-ICD患者既往获得的心脏ct资料。对危险器官、S-ICD组件和8节段(间隔)、11节段(外侧)和17节段(根尖)的假设规划靶体积(PTV)进行轮廓。对于每个患者和节段,计算了两种治疗方案,规定的PTV剂量为25 Gy:一种方案使S-ICD免受初级放疗束的影响(“幸免”),另一种方案没有这种限制(“非幸免”)。结果30个方案中有27个方案成功使S-ICD脱离主光束,D0.035cm3 < 1 Gy。在PTV与S-ICD之间距离4cm的三个备用平面图(PTV段11)中,D0.035cm3超过1gy。PTV第11段的备用方案与非备用方案相比,剂量/体积指标明显更高,计划质量降低(p < 0.05),尽管9/10方案在临床上仍可接受。PTV第8段和第17段无临床差异和统计学差异。结论S-ICD的存在并不是STAR的禁忌症,尽管侧段ptv可能会降低计划质量。罕见的PTV与S-ICD之间距离为4cm的病例可能会使放射治疗计划复杂化。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Physics and Imaging in Radiation Oncology
Physics and Astronomy-Radiation
CiteScore
5.30
自引率
18.90%
发文量
93
审稿时长
6 weeks
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


