Variation in coronary revascularisation and mortality after myocardial infarction across three public health insurance schemes in Thailand: an observational analysis from nationwide claims data.
Woranan Witthayapipopsakul, Orawan Anupraiwan, Gumpanart Veerakul, Anne Mills, Ipek Gurol-Urganci, Jan van der Meulen
{"title":"Variation in coronary revascularisation and mortality after myocardial infarction across three public health insurance schemes in Thailand: an observational analysis from nationwide claims data.","authors":"Woranan Witthayapipopsakul, Orawan Anupraiwan, Gumpanart Veerakul, Anne Mills, Ipek Gurol-Urganci, Jan van der Meulen","doi":"10.1136/bmjph-2024-001264","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Evidence on the impact of diverse healthcare insurance arrangements on healthcare variation is limited in low-income and middle-income countries. In Thailand, the Civil Servant Medical Benefit Scheme (CSMBS), Social Health Insurance (SHI) and Universal Coverage Scheme (UCS) have different provider choice and reimbursement arrangements and cover different populations. We explored to what extent use of revascularisation in patients with ST elevation myocardial infarction (STEMI) varied by insurance scheme.</p><p><strong>Methods: </strong>We used claims data, including all admissions for patients with STEMI between 2015 and 2020. Outcomes were any type of revascularisation, primary percutaneous coronary intervention (PPCI) and mortality. Regression models were used to estimate absolute differences (ADs) by scheme, adjusted for age, sex, comorbidities and admission year.</p><p><strong>Results: </strong>Of 98 142 patients, 75.7% were covered by UCS, 13.3% by CSMBS and 11.0% by SHI. Overall, 76.3% underwent revascularisation and 53.8% received PPCI. Mortality rates were 13.2% in-hospital and 20.7% at 180 days. Compared with UCS, use of revascularisation was slightly higher with CSMBS and slightly lower with SHI (AD: CSMBS 1.3% (95% CI -0.2 to 2.8), SHI -0.8% (-2.6 to 1.0), p=0.0264) and use of PPCI was slightly higher with CSMBS and SHI (AD: CSMBS 2.4% (-0.3 to 5.2), SHI 5.2% (3.1 to 7.2), p<0.0001)). CSMBS and SHI-insured patients had lower mortality compared with UCS (AD for in-hospital: CSMBS -1.3% (-2.1 to -0.5), SHI -0.9% (-1.8 to -0.1), p<0.0001; AD for 180-day mortality: CSMBS -4.5% (-5.3 to -3.6), SHI -1.9% (-3.0 to -0.8), p<0.0001). Effects of insurance scheme varied by hospital type for all outcomes (p for interaction<0.0001).</p><p><strong>Conclusion: </strong>Three-quarters of patients with STEMI received coronary revascularisation, suggesting potential undertreatment. We identified relatively small differences in access to revascularisation by insurance scheme which are unlikely to explain the lower mortality with CSMBS and SHI. Claims data can be used to assess the impact of insurance on access to effective treatments.</p>","PeriodicalId":101362,"journal":{"name":"BMJ public health","volume":"3 2","pages":"e001264"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12359411/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ public health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjph-2024-001264","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Evidence on the impact of diverse healthcare insurance arrangements on healthcare variation is limited in low-income and middle-income countries. In Thailand, the Civil Servant Medical Benefit Scheme (CSMBS), Social Health Insurance (SHI) and Universal Coverage Scheme (UCS) have different provider choice and reimbursement arrangements and cover different populations. We explored to what extent use of revascularisation in patients with ST elevation myocardial infarction (STEMI) varied by insurance scheme.
Methods: We used claims data, including all admissions for patients with STEMI between 2015 and 2020. Outcomes were any type of revascularisation, primary percutaneous coronary intervention (PPCI) and mortality. Regression models were used to estimate absolute differences (ADs) by scheme, adjusted for age, sex, comorbidities and admission year.
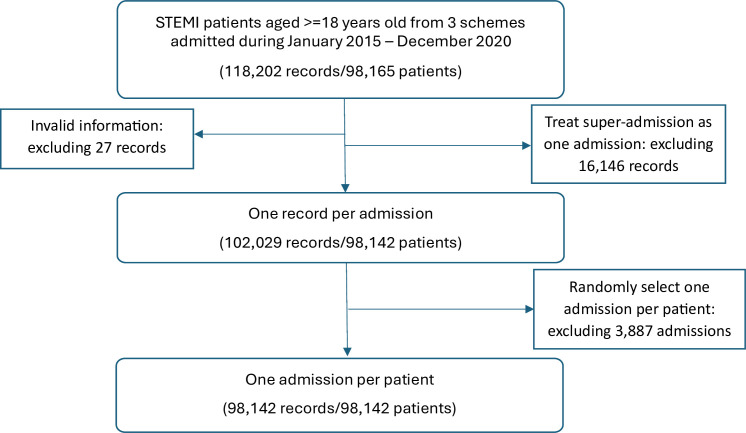
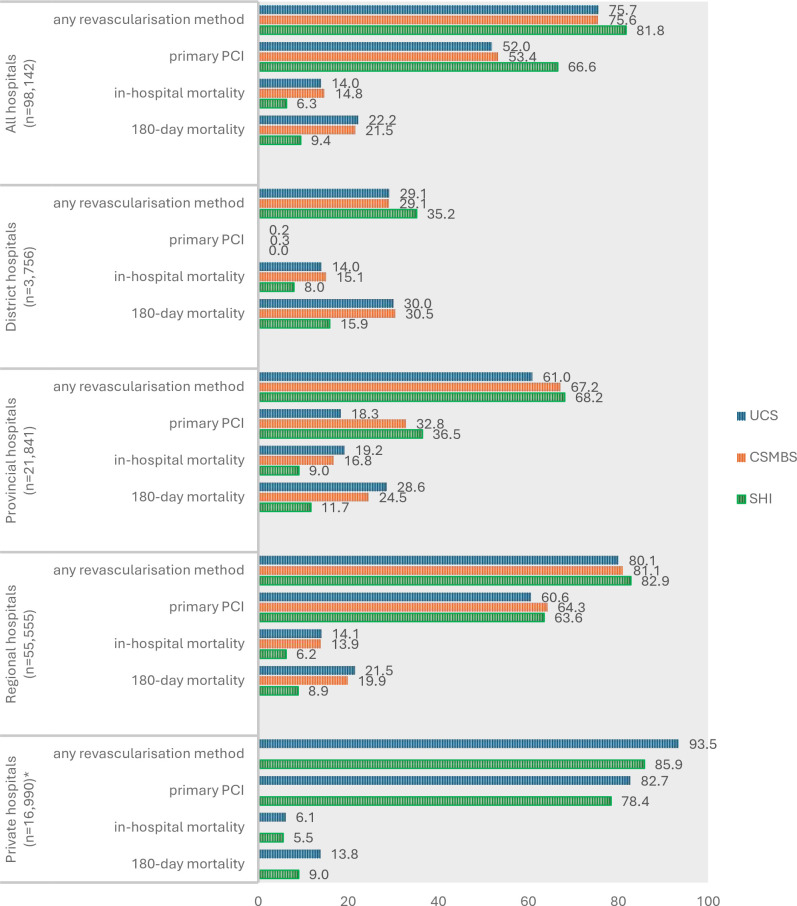
Results: Of 98 142 patients, 75.7% were covered by UCS, 13.3% by CSMBS and 11.0% by SHI. Overall, 76.3% underwent revascularisation and 53.8% received PPCI. Mortality rates were 13.2% in-hospital and 20.7% at 180 days. Compared with UCS, use of revascularisation was slightly higher with CSMBS and slightly lower with SHI (AD: CSMBS 1.3% (95% CI -0.2 to 2.8), SHI -0.8% (-2.6 to 1.0), p=0.0264) and use of PPCI was slightly higher with CSMBS and SHI (AD: CSMBS 2.4% (-0.3 to 5.2), SHI 5.2% (3.1 to 7.2), p<0.0001)). CSMBS and SHI-insured patients had lower mortality compared with UCS (AD for in-hospital: CSMBS -1.3% (-2.1 to -0.5), SHI -0.9% (-1.8 to -0.1), p<0.0001; AD for 180-day mortality: CSMBS -4.5% (-5.3 to -3.6), SHI -1.9% (-3.0 to -0.8), p<0.0001). Effects of insurance scheme varied by hospital type for all outcomes (p for interaction<0.0001).
Conclusion: Three-quarters of patients with STEMI received coronary revascularisation, suggesting potential undertreatment. We identified relatively small differences in access to revascularisation by insurance scheme which are unlikely to explain the lower mortality with CSMBS and SHI. Claims data can be used to assess the impact of insurance on access to effective treatments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


