Meng-Yu Wu, Giou-Teng Yiang, Sy-Jou Chen, Hon-Ping Ma, Mau-Roung Lin
{"title":"Influence of on-scene time and prehospital interventions on inhospital mortality in trauma patients.","authors":"Meng-Yu Wu, Giou-Teng Yiang, Sy-Jou Chen, Hon-Ping Ma, Mau-Roung Lin","doi":"10.1186/s12873-025-01324-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study aimed to investigate the impact of the type and number of prehospital interventions, in addition to prehospital time intervals, on inhospital mortality among trauma patients.</p><p><strong>Methods: </strong>According to a 13-year prospective trauma registry, three prehospital time intervals of response time, on-scene time, and transport time were assessed. Prehospital interventions were classified into four categories: stop bleeding strategies, immobilization, basic airway management, and advanced resuscitation.</p><p><strong>Results: </strong>A total of 13,533 patients were included. Relative to patients not receiving prehospital interventions, there was longer on-scene time for those who received immobilization (10.4 vs. 8.68 min), basic airway management (11.4 vs. 9.40 min), and advanced resuscitation (12.6 vs. 9.53 min). Furthermore, relative to patients who survived in hospital, those who died significantly had longer on-scene time (11.4 vs. 9.64 min) and sustained immobilization (74.7% vs. 52.5%), basic airway management (30.7% vs. 7.6%), advanced resuscitation (32.0% vs. 0.1%), and ≥ 4 prehospital interventions (30.4% vs. 4.6%). Results of the multivariable logistic regression analysis shows that without adjustment for type and number of prehospital interventions, longer on-scene time (odds ratio [OR] = 1.03; 95% confidence interval [CI], 1.01-1.04) were significantly associated with increased mortality; however, after additional adjustment for type and number of prehospital interventions, no significant association between each of the three prehospital time intervals and mortality was detected. Furthermore, compared to patients who did not receive prehospital interventions, those who received wound packing/compression had a significantly lower risk of mortality (OR = 0.54; 95% CI, 0.36-0.80), whereas those who received basic airway management (OR = 1.73; 95% CI, 1.15-2.60), advanced resuscitation (OR = 33.4; 95% CI, 14.9-75.0), and three (OR = 2.60; 95% CI, 1.01-6.93) and ≥ 4 (OR = 2.97; 95% CI, 1.01-9.63) prehospital interventions had a significantly higher risk of mortality.</p><p><strong>Conclusions: </strong>There exists a tradeoff between prehospital trauma interventions and shortening on-scene time for mortality risk; however, implementing some interventions for hemorrhage control and hemostatic resuscitation can benefit the survival of trauma patients the most.</p><p><strong>Clinical trial number: </strong>Not applicable.</p>","PeriodicalId":9002,"journal":{"name":"BMC Emergency Medicine","volume":"25 1","pages":"163"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12366050/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12873-025-01324-7","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: This study aimed to investigate the impact of the type and number of prehospital interventions, in addition to prehospital time intervals, on inhospital mortality among trauma patients.
Methods: According to a 13-year prospective trauma registry, three prehospital time intervals of response time, on-scene time, and transport time were assessed. Prehospital interventions were classified into four categories: stop bleeding strategies, immobilization, basic airway management, and advanced resuscitation.
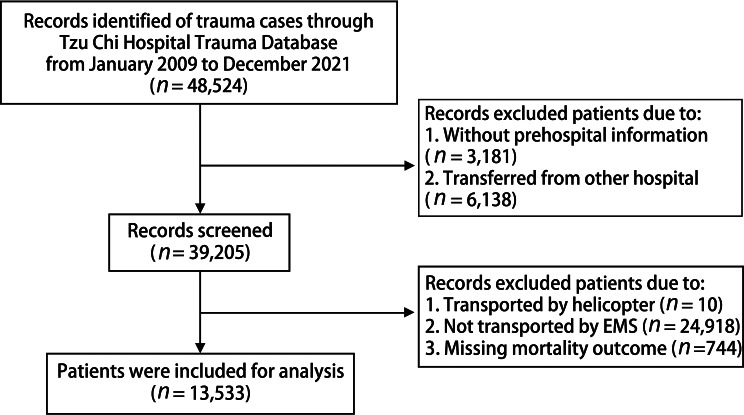
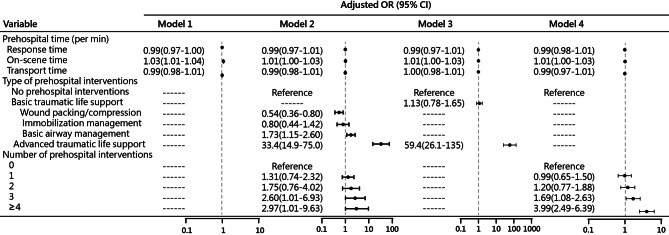
Results: A total of 13,533 patients were included. Relative to patients not receiving prehospital interventions, there was longer on-scene time for those who received immobilization (10.4 vs. 8.68 min), basic airway management (11.4 vs. 9.40 min), and advanced resuscitation (12.6 vs. 9.53 min). Furthermore, relative to patients who survived in hospital, those who died significantly had longer on-scene time (11.4 vs. 9.64 min) and sustained immobilization (74.7% vs. 52.5%), basic airway management (30.7% vs. 7.6%), advanced resuscitation (32.0% vs. 0.1%), and ≥ 4 prehospital interventions (30.4% vs. 4.6%). Results of the multivariable logistic regression analysis shows that without adjustment for type and number of prehospital interventions, longer on-scene time (odds ratio [OR] = 1.03; 95% confidence interval [CI], 1.01-1.04) were significantly associated with increased mortality; however, after additional adjustment for type and number of prehospital interventions, no significant association between each of the three prehospital time intervals and mortality was detected. Furthermore, compared to patients who did not receive prehospital interventions, those who received wound packing/compression had a significantly lower risk of mortality (OR = 0.54; 95% CI, 0.36-0.80), whereas those who received basic airway management (OR = 1.73; 95% CI, 1.15-2.60), advanced resuscitation (OR = 33.4; 95% CI, 14.9-75.0), and three (OR = 2.60; 95% CI, 1.01-6.93) and ≥ 4 (OR = 2.97; 95% CI, 1.01-9.63) prehospital interventions had a significantly higher risk of mortality.
Conclusions: There exists a tradeoff between prehospital trauma interventions and shortening on-scene time for mortality risk; however, implementing some interventions for hemorrhage control and hemostatic resuscitation can benefit the survival of trauma patients the most.
期刊介绍:
BMC Emergency Medicine is an open access, peer-reviewed journal that considers articles on all urgent and emergency aspects of medicine, in both practice and basic research. In addition, the journal covers aspects of disaster medicine and medicine in special locations, such as conflict areas and military medicine, together with articles concerning healthcare services in the emergency departments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


