Marilyn J Manco-Johnson, Binh Le, Suchitra Acharya, Sanjay Ahuja, Meera Chitlur, Divyaswathi Citla-Sridhar, Stacey Ann Fedewa, Daniel Isaac, Roshni Kulkarni, Laura A Schieve, Anjali Sharathkumar, J Michael Soucie
{"title":"Risk factors for joint bleeding in severe hemophilia A and B: analysis of the Community Counts longitudinal surveillance cohort.","authors":"Marilyn J Manco-Johnson, Binh Le, Suchitra Acharya, Sanjay Ahuja, Meera Chitlur, Divyaswathi Citla-Sridhar, Stacey Ann Fedewa, Daniel Isaac, Roshni Kulkarni, Laura A Schieve, Anjali Sharathkumar, J Michael Soucie","doi":"10.1016/j.bvth.2025.100047","DOIUrl":null,"url":null,"abstract":"<p><p>Joint bleeding is the primary determinant of end-stage arthropathy in hemophilia; joint bleeding has greatly decreased with the use of prophylaxis and introduction of highly effective therapies. This study aimed to determine current risk factors for joint bleeding in persons with severe hemophilia A or B. Demographic, treatment, and bleeding outcome data from Community Counts, a US national surveillance project, were analyzed. Data were collected at annual visits between 2013 and 2022. Eligibility included factor VIII or IX of <1%, no inhibitor, age of 2 to 44 years, and on treatment with continuous prophylaxis. Annual joint bleeding rate (AJBR) differences across demographic and clinical subgroups were compared via rate ratios and 95% confidence intervals, and with multivariate methods accounting for multiple measurements over time. The analysis included 2527 males with hemophilia, 7211 observation years, and 10 046 joint bleeds. Lower AJBR in hemophilia A was most strongly associated with use of emicizumab. For both hemophilia A and B, patient-associated factors, younger age, fewer missed doses, and full employment were all independently associated with lower AJBR, as was treatment in the Northeast of the United States. The findings of this comprehensive analysis of a large, diverse sample drawn from hemophilia treatment centers across the United States, underscore the important contributions of patient, community, and treatment factors on joint outcomes in severe hemophilia. Use of emicizumab and few missed doses independently predicted low AJBR, highlighting the interplay of access and adherence to care.</p>","PeriodicalId":100190,"journal":{"name":"Blood Vessels, Thrombosis & Hemostasis","volume":"2 3","pages":"100047"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12356300/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood Vessels, Thrombosis & Hemostasis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.bvth.2025.100047","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
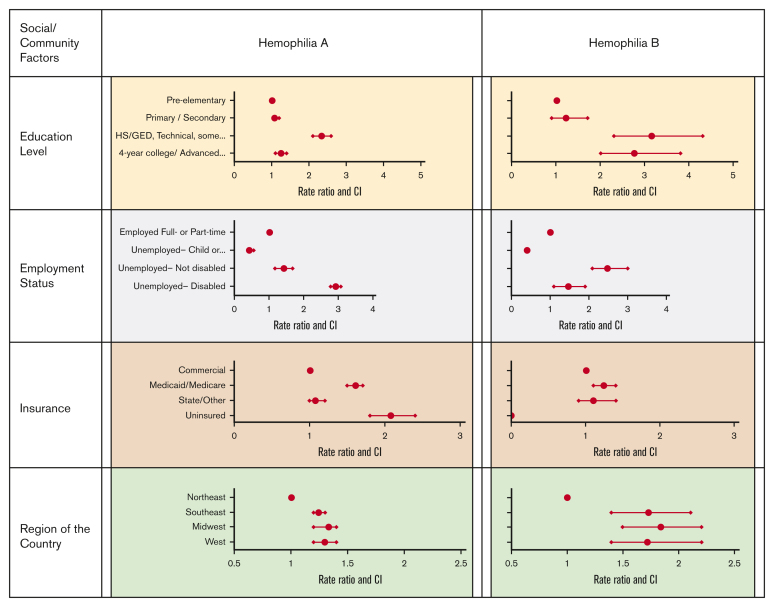
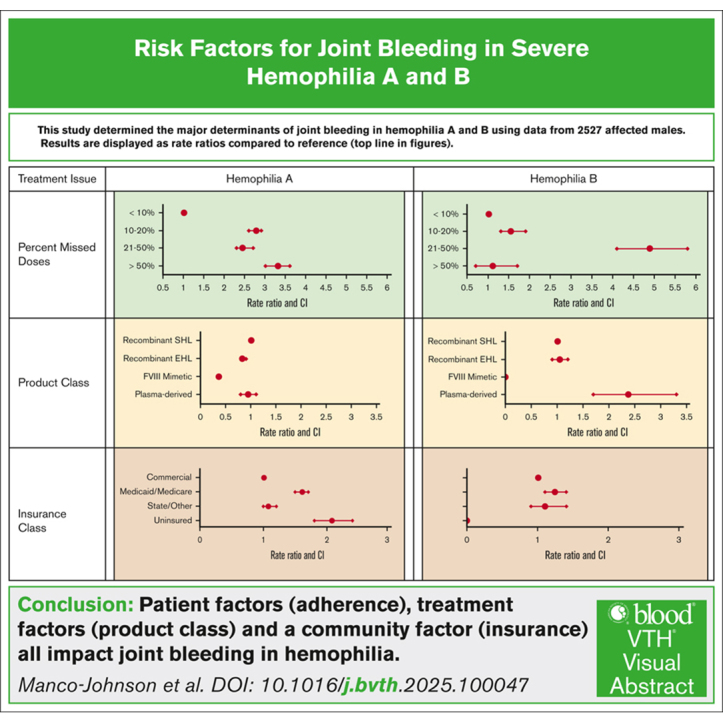
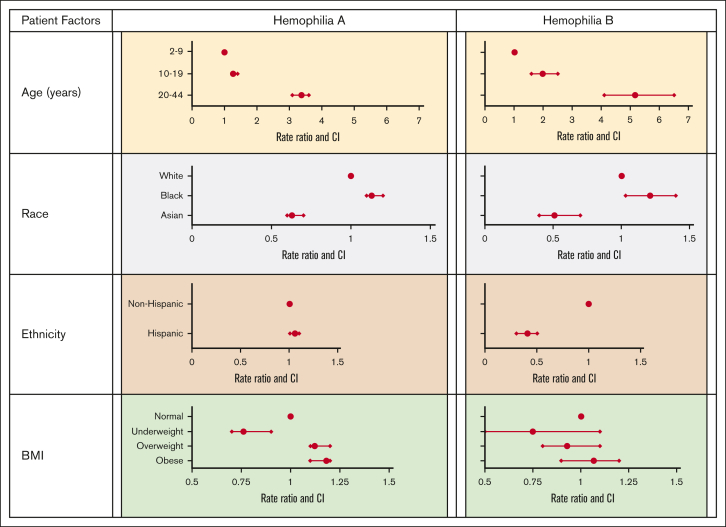
Joint bleeding is the primary determinant of end-stage arthropathy in hemophilia; joint bleeding has greatly decreased with the use of prophylaxis and introduction of highly effective therapies. This study aimed to determine current risk factors for joint bleeding in persons with severe hemophilia A or B. Demographic, treatment, and bleeding outcome data from Community Counts, a US national surveillance project, were analyzed. Data were collected at annual visits between 2013 and 2022. Eligibility included factor VIII or IX of <1%, no inhibitor, age of 2 to 44 years, and on treatment with continuous prophylaxis. Annual joint bleeding rate (AJBR) differences across demographic and clinical subgroups were compared via rate ratios and 95% confidence intervals, and with multivariate methods accounting for multiple measurements over time. The analysis included 2527 males with hemophilia, 7211 observation years, and 10 046 joint bleeds. Lower AJBR in hemophilia A was most strongly associated with use of emicizumab. For both hemophilia A and B, patient-associated factors, younger age, fewer missed doses, and full employment were all independently associated with lower AJBR, as was treatment in the Northeast of the United States. The findings of this comprehensive analysis of a large, diverse sample drawn from hemophilia treatment centers across the United States, underscore the important contributions of patient, community, and treatment factors on joint outcomes in severe hemophilia. Use of emicizumab and few missed doses independently predicted low AJBR, highlighting the interplay of access and adherence to care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


