Summer M Drees, Cade R McGarvey, Noah Miller, Sahil Kapur, Anderson Lee, Martin Skie, Ahmed Suparno Bahar Moni
{"title":"Trans-Ulnar Single Incision Fasciotomy for Decompression of Forearm Compartment Syndrome: A Cadaveric Study.","authors":"Summer M Drees, Cade R McGarvey, Noah Miller, Sahil Kapur, Anderson Lee, Martin Skie, Ahmed Suparno Bahar Moni","doi":"10.1111/os.70157","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Acute compartment syndrome (ACS) is a medical emergency that requires timely intervention, and delays in treatment can lead to severe complications such as nerve injury, muscle necrosis, amputation, and even death. Definitive treatment of ACS requires a fasciotomy. Currently, there is no consensus on the best approach for a forearm fasciotomy; compartment release is most commonly done through volar or combined volar and dorsal incisions. A trans-ulnar single incision approach has been demonstrated to be effective in a case report. This study investigates if a trans-ulnar single incision decompresses both deep volar and dorsal forearm compartments to less than 30 mmHg in a cadaveric model of ACS.</p><p><strong>Methods: </strong>Ten fresh, frozen cadaveric upper extremities were injected with egg whites and compartment pressures were measured to determine successful simulation of ACS. A single trans-ulnar incision was made between the Flexor Carpi Ulnaris (FCU) and Extensor Carpi Ulnaris (ECU), extending from 4 to 5 cm (2″) proximal to the ulnar styloid to 6 to 8 cm (3″) distal to the olecranon. After blunt dissection to release the compartments, pressures were measured to confirm decompression.</p><p><strong>Results: </strong>ACS was successfully simulated in all upper extremities to above 30 mmHg. The mean volume of saline injected to simulate local anesthetic was 38.0 ± 4.2 mL. The mean operative time was 10.1 min. The mean compartment readings 1-min post-fasciotomy were 7.1 ± 3.0 mmHg for the deep volar compartment and 9.4 ± 5.6 mmHg for the dorsal compartment. All fasciotomies reduced deep volar and dorsal compartment pressures below the clinical threshold of 30 mmHg, with significant differences between pre- and post-fasciotomy pressures.</p><p><strong>Conclusions: </strong>All 10 fasciotomies successfully reduced deep volar and dorsal compartment pressures to below the clinical threshold of 30 mmHg, demonstrating the success of the trans-ulnar single incision fasciotomy to decompress compartment syndrome in cadaveric forearms.</p>","PeriodicalId":19566,"journal":{"name":"Orthopaedic Surgery","volume":" ","pages":"2982-2991"},"PeriodicalIF":2.1000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12497538/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Orthopaedic Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/os.70157","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/18 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Acute compartment syndrome (ACS) is a medical emergency that requires timely intervention, and delays in treatment can lead to severe complications such as nerve injury, muscle necrosis, amputation, and even death. Definitive treatment of ACS requires a fasciotomy. Currently, there is no consensus on the best approach for a forearm fasciotomy; compartment release is most commonly done through volar or combined volar and dorsal incisions. A trans-ulnar single incision approach has been demonstrated to be effective in a case report. This study investigates if a trans-ulnar single incision decompresses both deep volar and dorsal forearm compartments to less than 30 mmHg in a cadaveric model of ACS.
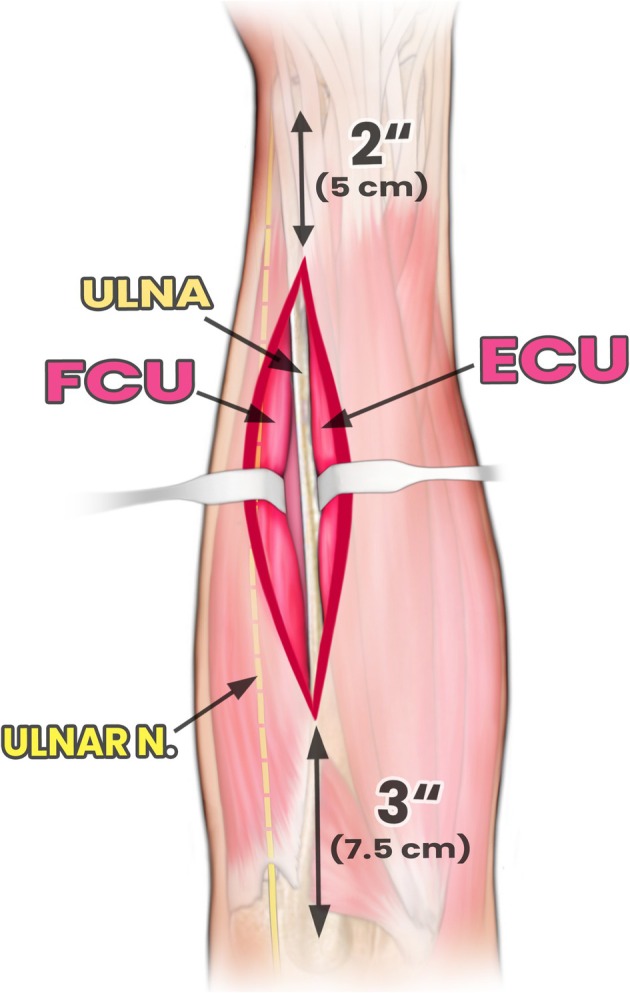
Methods: Ten fresh, frozen cadaveric upper extremities were injected with egg whites and compartment pressures were measured to determine successful simulation of ACS. A single trans-ulnar incision was made between the Flexor Carpi Ulnaris (FCU) and Extensor Carpi Ulnaris (ECU), extending from 4 to 5 cm (2″) proximal to the ulnar styloid to 6 to 8 cm (3″) distal to the olecranon. After blunt dissection to release the compartments, pressures were measured to confirm decompression.
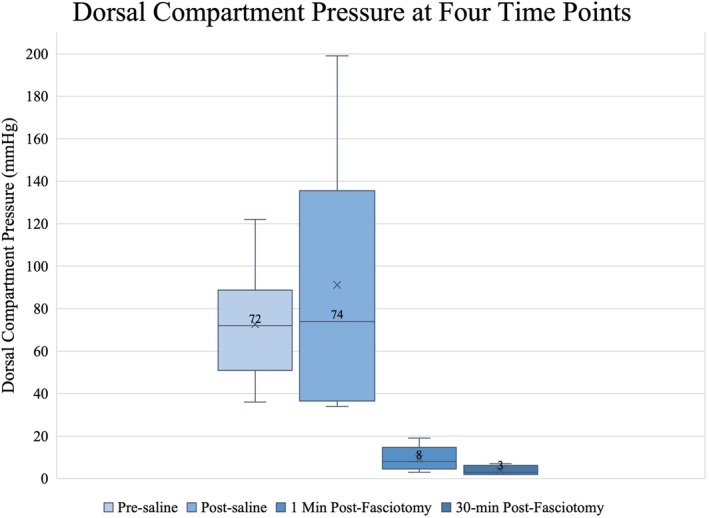
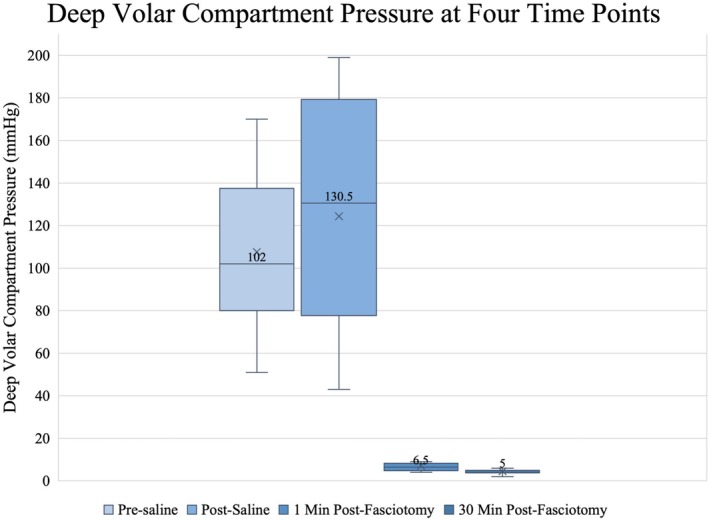
Results: ACS was successfully simulated in all upper extremities to above 30 mmHg. The mean volume of saline injected to simulate local anesthetic was 38.0 ± 4.2 mL. The mean operative time was 10.1 min. The mean compartment readings 1-min post-fasciotomy were 7.1 ± 3.0 mmHg for the deep volar compartment and 9.4 ± 5.6 mmHg for the dorsal compartment. All fasciotomies reduced deep volar and dorsal compartment pressures below the clinical threshold of 30 mmHg, with significant differences between pre- and post-fasciotomy pressures.
Conclusions: All 10 fasciotomies successfully reduced deep volar and dorsal compartment pressures to below the clinical threshold of 30 mmHg, demonstrating the success of the trans-ulnar single incision fasciotomy to decompress compartment syndrome in cadaveric forearms.
期刊介绍:
Orthopaedic Surgery (OS) is the official journal of the Chinese Orthopaedic Association, focusing on all aspects of orthopaedic technique and surgery.
The journal publishes peer-reviewed articles in the following categories: Original Articles, Clinical Articles, Review Articles, Guidelines, Editorials, Commentaries, Surgical Techniques, Case Reports and Meeting Reports.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


