Samantha L Hocking, David A Scott, Matthew L Remedios, Michael Horowitz, David A Story, Jerry R Greenfield, Alex Boussioutas, Benedict Devereaux, Sofianos Andrikopoulos, Jonathan E Shaw, Benjamin L Olesnicky
{"title":"2025 ADS/ANZCA/GESA/NACOS clinical practice recommendations on the peri-procedural use of GLP-1/GIP receptor agonists.","authors":"Samantha L Hocking, David A Scott, Matthew L Remedios, Michael Horowitz, David A Story, Jerry R Greenfield, Alex Boussioutas, Benedict Devereaux, Sofianos Andrikopoulos, Jonathan E Shaw, Benjamin L Olesnicky","doi":"10.1177/0310057X251355288","DOIUrl":null,"url":null,"abstract":"<p><p>Glucagon-like peptide-1 receptor agonists (GLP-1RAs) are widely used for the treatment of type 2 diabetes and/or obesity. The physiological actions of endogenous GLP-1, and synthetic GLP-1RAs include inhibition of gastric emptying. This has peri-procedural implications due to the potential increased risk of retained gastric contents which may result in pulmonary aspiration. There is a need for local evidence-based guidelines to best manage patients on GLP-1RAs and dual GLP-1 and glucose-dependent insulinotropic polypeptide receptor co-agonists (GLP-1/GIPRAs) presenting for surgical and medical procedures requiring sedation or anaesthesia. A panel of experts was formed to consider the peri-procedural implications of GLP-1RA and GLP-1/GIPRA use and establish best practice recommendations based on the current evidence.We recommend that all patients should be asked about glucagon-like peptide-1 receptor agonist (GLP-1RA) and dual GLP-1 and glucose-dependent insulinotropic polypeptide receptor co-agonist (GLP-1/GIPRA) use prior to anaesthesia or sedation for surgical and endoscopic procedures and be informed of the benefits and risks. We also recommend that GLP-1RAs and GLP-1/GIPRAs be continued in the peri-procedural period. Preprocedural diet modification with a 24-h clear fluid diet, followed by standard 6-h fasting, should be recommended for all patients receiving GLP-1RAs or GLP-1/GIPRAs. In patients who have not completed or are unable to have a 24-h liquid diet, risk stratification using gastric ultrasound or minimally sedated gastroscopy to assess gastric contents is recommended, as is the use of intravenous erythromycin. We cannot currently recommend using the absence of gastrointestinal symptoms for risk stratification, nor can we recommend an adequate cessation period for GLP-1RAs and GLP-1/GIPRAs to ensure gastric emptying has returned to baseline levels. This clinical guideline, developed by multiple professional bodies, outlines current best practice recommendations for patients taking GLP-1RAs and combined GLP-1/GIPRAs who require general anaesthesia, sedation and/or endoscopic procedures. The guide provides a structure for Australian and New Zealand primary health practitioners, gastroenterologists, surgeons, endocrinologists, anaesthetists and perioperative physicians to support clinical decisions in these patients.</p>","PeriodicalId":7746,"journal":{"name":"Anaesthesia and Intensive Care","volume":" ","pages":"300-306"},"PeriodicalIF":1.2000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12420935/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anaesthesia and Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/0310057X251355288","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/14 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
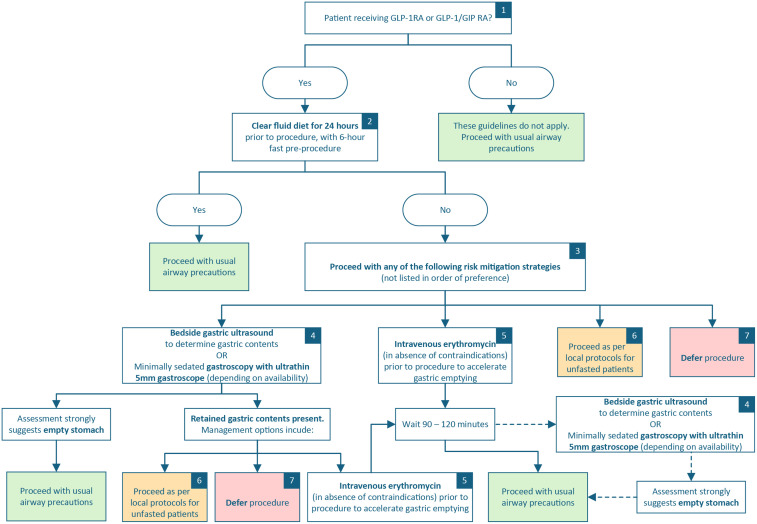
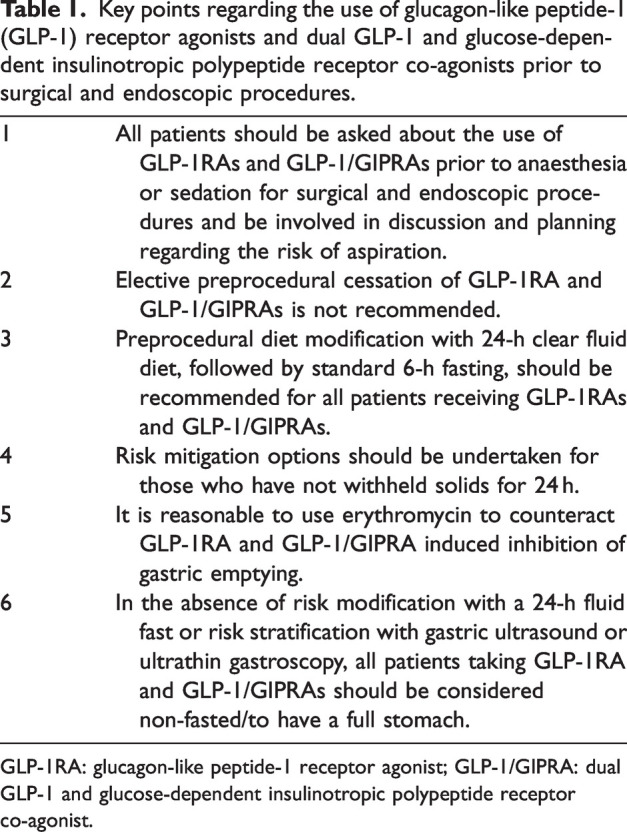
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) are widely used for the treatment of type 2 diabetes and/or obesity. The physiological actions of endogenous GLP-1, and synthetic GLP-1RAs include inhibition of gastric emptying. This has peri-procedural implications due to the potential increased risk of retained gastric contents which may result in pulmonary aspiration. There is a need for local evidence-based guidelines to best manage patients on GLP-1RAs and dual GLP-1 and glucose-dependent insulinotropic polypeptide receptor co-agonists (GLP-1/GIPRAs) presenting for surgical and medical procedures requiring sedation or anaesthesia. A panel of experts was formed to consider the peri-procedural implications of GLP-1RA and GLP-1/GIPRA use and establish best practice recommendations based on the current evidence.We recommend that all patients should be asked about glucagon-like peptide-1 receptor agonist (GLP-1RA) and dual GLP-1 and glucose-dependent insulinotropic polypeptide receptor co-agonist (GLP-1/GIPRA) use prior to anaesthesia or sedation for surgical and endoscopic procedures and be informed of the benefits and risks. We also recommend that GLP-1RAs and GLP-1/GIPRAs be continued in the peri-procedural period. Preprocedural diet modification with a 24-h clear fluid diet, followed by standard 6-h fasting, should be recommended for all patients receiving GLP-1RAs or GLP-1/GIPRAs. In patients who have not completed or are unable to have a 24-h liquid diet, risk stratification using gastric ultrasound or minimally sedated gastroscopy to assess gastric contents is recommended, as is the use of intravenous erythromycin. We cannot currently recommend using the absence of gastrointestinal symptoms for risk stratification, nor can we recommend an adequate cessation period for GLP-1RAs and GLP-1/GIPRAs to ensure gastric emptying has returned to baseline levels. This clinical guideline, developed by multiple professional bodies, outlines current best practice recommendations for patients taking GLP-1RAs and combined GLP-1/GIPRAs who require general anaesthesia, sedation and/or endoscopic procedures. The guide provides a structure for Australian and New Zealand primary health practitioners, gastroenterologists, surgeons, endocrinologists, anaesthetists and perioperative physicians to support clinical decisions in these patients.
期刊介绍:
Anaesthesia and Intensive Care is an international journal publishing timely, peer reviewed articles that have educational value and scientific merit for clinicians and researchers associated with anaesthesia, intensive care medicine, and pain medicine.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


