Mehmet A Bilen, Brandon Diessner, John White, Louise Murphy, Amy Nguyen, Melissa Kirker, Norbek Gharibian, Valerie Morris, Abhijeet Bhanegaonkar
{"title":"Impact of treatment patterns and sequencing on clinical and economic outcomes in patients with metastatic urothelial cancer: IMPACT UC II study.","authors":"Mehmet A Bilen, Brandon Diessner, John White, Louise Murphy, Amy Nguyen, Melissa Kirker, Norbek Gharibian, Valerie Morris, Abhijeet Bhanegaonkar","doi":"10.1093/oncolo/oyaf249","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Real-world data about treatment sequencing and economic and clinical outcomes in patients with metastatic urothelial cancer (mUC) are limited.</p><p><strong>Objective: </strong>The IMPACT UC II study evaluated real-world overall survival (OS), first-line (1L) to second-line (2L) progression, and healthcare resource utilization (HCRU) and costs in patients with mUC before US approval of avelumab 1L maintenance in June 2020.</p><p><strong>Design: </strong>Retrospective study.</p><p><strong>Setting: </strong>US insurance claims data from the Optum Research Database.</p><p><strong>Participants: </strong>Adults diagnosed with mUC from July 2015 to June 2020, observed until death, disenrollment, or study end (August 2021).</p><p><strong>Intervention(s) or exposure(s): </strong>Three cohorts were defined based on 1L treatment received: cisplatin-based chemotherapy, carboplatin-based chemotherapy, or immuno-oncology (IO) monotherapy.</p><p><strong>Main outcome(s) and measure(s): </strong>Analyses included OS (multivariable Cox proportional hazards),1L-to-2L progression (incidence rates), HCRU and costs (medians), and multivariable-adjusted cumulative 24-month predicted costs (Lin regression models).</p><p><strong>Results: </strong>Of 3006 patients with mUC, 1037 received 1L treatment: cisplatin-based in 365 (35.2%), carboplatin-based in 337 (32.5%), and IO in 335 (32.3%). Compared with 1L cisplatin-based chemotherapy, mortality risk (hazard ratio [95% CI]) was doubled with IO monotherapy (2.0 [1.6-2.5]) and 1.5-times higher with carboplatin-based chemotherapy (1.5 [1.3-1.9]). The 1L-to-2L progression rate per 100 person-years was highest in patients receiving carboplatin-based chemotherapy (74.4) compared with cisplatin-based chemotherapy (51.9) and IO monotherapy (29.8). All-cause HCRU was lowest with carboplatin-based chemotherapy. Median all-cause and mUC-related costs were highest with IO monotherapy (mUC-related per patient per month: IO, $9739; cisplatin-based, $6687; carboplatin-based, $5219) as were cumulative 24-month predicted costs (mUC-related: IO, $157 595; cisplatin-based $122 351; carboplatin-based, $112 412).</p><p><strong>Conclusions: </strong>Approximately one-third of patients with mUC in this population received 1L therapy. Mortality, HCRU, and costs were higher with IO monotherapy vs platinum-based chemotherapy.</p><p><strong>Relevance: </strong>Results provide baseline data for future studies evaluating the impact of newer treatment options for patients with mUC.</p>","PeriodicalId":54686,"journal":{"name":"Oncologist","volume":" ","pages":""},"PeriodicalIF":4.2000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12517744/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Oncologist","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/oncolo/oyaf249","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: Real-world data about treatment sequencing and economic and clinical outcomes in patients with metastatic urothelial cancer (mUC) are limited.
Objective: The IMPACT UC II study evaluated real-world overall survival (OS), first-line (1L) to second-line (2L) progression, and healthcare resource utilization (HCRU) and costs in patients with mUC before US approval of avelumab 1L maintenance in June 2020.
Design: Retrospective study.
Setting: US insurance claims data from the Optum Research Database.
Participants: Adults diagnosed with mUC from July 2015 to June 2020, observed until death, disenrollment, or study end (August 2021).
Intervention(s) or exposure(s): Three cohorts were defined based on 1L treatment received: cisplatin-based chemotherapy, carboplatin-based chemotherapy, or immuno-oncology (IO) monotherapy.
Main outcome(s) and measure(s): Analyses included OS (multivariable Cox proportional hazards),1L-to-2L progression (incidence rates), HCRU and costs (medians), and multivariable-adjusted cumulative 24-month predicted costs (Lin regression models).
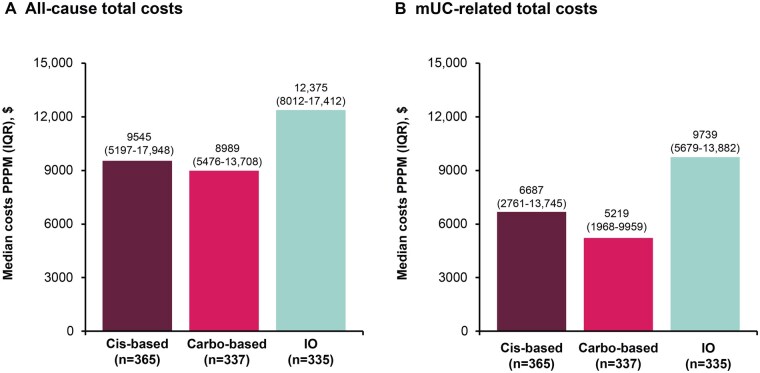
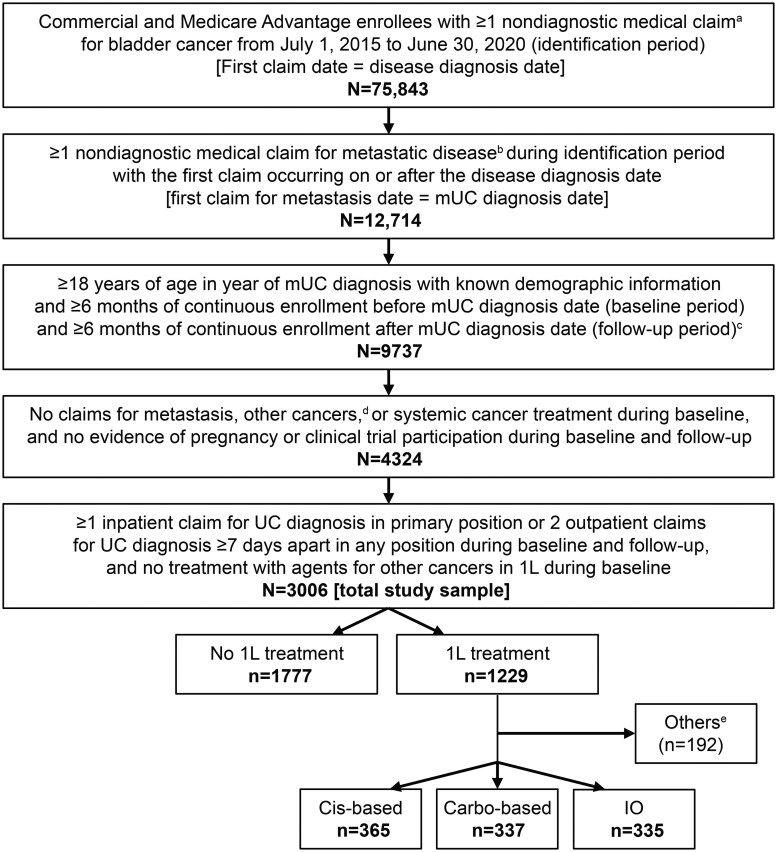
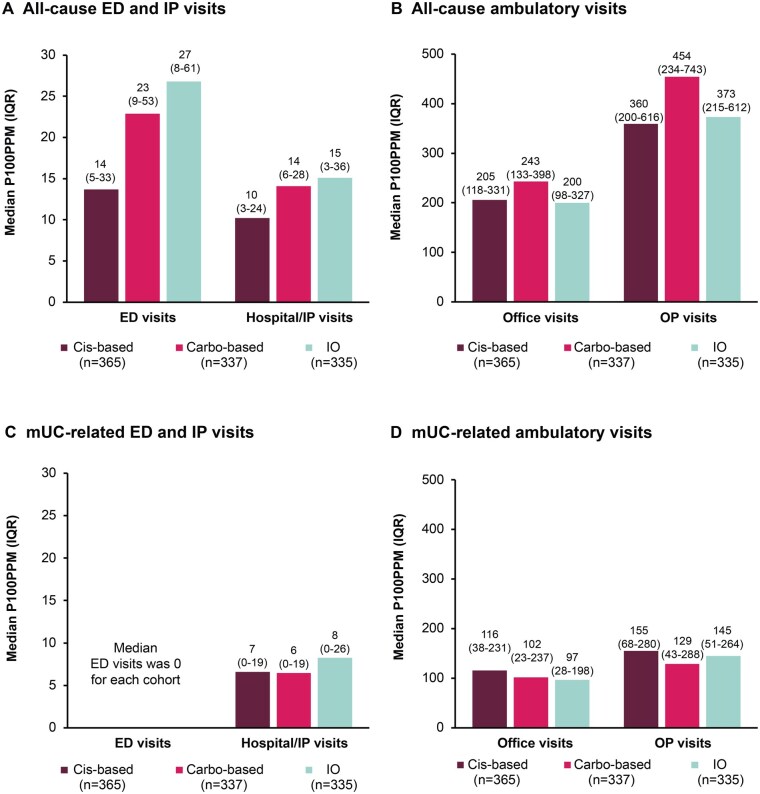
Results: Of 3006 patients with mUC, 1037 received 1L treatment: cisplatin-based in 365 (35.2%), carboplatin-based in 337 (32.5%), and IO in 335 (32.3%). Compared with 1L cisplatin-based chemotherapy, mortality risk (hazard ratio [95% CI]) was doubled with IO monotherapy (2.0 [1.6-2.5]) and 1.5-times higher with carboplatin-based chemotherapy (1.5 [1.3-1.9]). The 1L-to-2L progression rate per 100 person-years was highest in patients receiving carboplatin-based chemotherapy (74.4) compared with cisplatin-based chemotherapy (51.9) and IO monotherapy (29.8). All-cause HCRU was lowest with carboplatin-based chemotherapy. Median all-cause and mUC-related costs were highest with IO monotherapy (mUC-related per patient per month: IO, $9739; cisplatin-based, $6687; carboplatin-based, $5219) as were cumulative 24-month predicted costs (mUC-related: IO, $157 595; cisplatin-based $122 351; carboplatin-based, $112 412).
Conclusions: Approximately one-third of patients with mUC in this population received 1L therapy. Mortality, HCRU, and costs were higher with IO monotherapy vs platinum-based chemotherapy.
Relevance: Results provide baseline data for future studies evaluating the impact of newer treatment options for patients with mUC.
期刊介绍:
The Oncologist® is dedicated to translating the latest research developments into the best multidimensional care for cancer patients. Thus, The Oncologist is committed to helping physicians excel in this ever-expanding environment through the publication of timely reviews, original studies, and commentaries on important developments. We believe that the practice of oncology requires both an understanding of a range of disciplines encompassing basic science related to cancer, translational research, and clinical practice, but also the socioeconomic and psychosocial factors that determine access to care and quality of life and function following cancer treatment.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


