Circumferential pulmonary vein isolation with adjunctive linear ablation vs. circumferential pulmonary vein isolation alone for long-standing persistent atrial fibrillation: a randomized pilot study.
Yeqian Zhu, Yan Dong, Qiushi Chen, Li Jiang, Yuan He, Nishant Yadav, Kejiang Cao, Fengxiang Zhang
{"title":"Circumferential pulmonary vein isolation with adjunctive linear ablation vs. circumferential pulmonary vein isolation alone for long-standing persistent atrial fibrillation: a randomized pilot study.","authors":"Yeqian Zhu, Yan Dong, Qiushi Chen, Li Jiang, Yuan He, Nishant Yadav, Kejiang Cao, Fengxiang Zhang","doi":"10.1093/europace/euaf176","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>This prospective randomized controlled trial investigated the comparative efficacy and safety of circumferential pulmonary vein isolation (CPVI) combined with modified linear ablation (CPVI-MLA) vs. standalone CPVI in patients with long-standing persistent atrial fibrillation (LSPAF).</p><p><strong>Methods and results: </strong>In this single-centre pilot trial, 134 LSPAF patients were randomized to the CPVI-MLA (n = 67) or CPVI-only (n = 67) groups. The CPVI-MLA protocol integrated four components: (i) ethanol infusion targeting the ligament of Marshall; (ii) complete CPVI; (iii) extended lesion sets (posterior wall isolation, dual isthmus ablation); and (iv) substrate modification [left atrial intima adjoining coronary sinus (LAI-CS) and superior vena cava isolation (SVCI)]. A 24 h Holter monitoring was performed at the 1st, 3rd, and 6th month follow-up visits, with 7-day Holter monitoring at the 12th month follow-up visit. The primary endpoint was freedom from atrial tachyarrhythmias (≥ 30 s) after the initial 3-month blanking period post-index procedure, without antiarrhythmic drugs. After a mean follow-up of 14.5 ± 9.1 months, 76.1% (51/67) in the CPVI-MLA group and 65.7% (44/67) in the CPVI-only group achieved the primary endpoint (P = 0.32). However, the CPVI-MLA group demonstrated significantly higher atrial fibrillation (AF)-free survival rate (91.0 vs. 76.1%, P = 0.049), while atrial tachycardia/atrial flutter-free survival rates were comparable (83.5 vs. 88.1%, P = 0.45). The CPVI-MLA strategy required longer ablation time (68.6 ± 12.3 vs. 49.4 ± 10.3 min, P < 0.001) and fluoroscopy exposure (14.9 ± 9.8 vs. 9.3 ± 6.7 min, P < 0.001). Serious adverse events were rare and similar between groups (1.5 vs. 0%, P = 1.00).</p><p><strong>Conclusion: </strong>In patients with LSPAF, the CPVI-MLA strategy significantly improved freedom from AF compared with CPVI alone, although it did not improve overall sinus rhythm maintenance rate. This strategy may offer a refined approach for complex AF ablation, warranting further validation in larger trials.</p>","PeriodicalId":11981,"journal":{"name":"Europace","volume":" ","pages":""},"PeriodicalIF":7.4000,"publicationDate":"2025-08-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12395555/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Europace","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/europace/euaf176","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
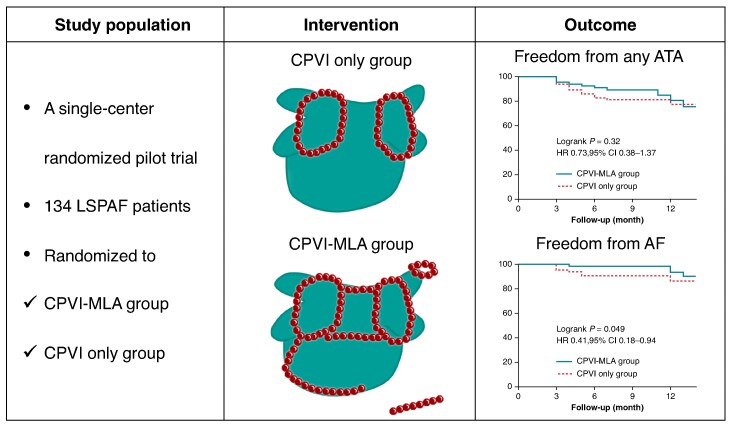
Aims: This prospective randomized controlled trial investigated the comparative efficacy and safety of circumferential pulmonary vein isolation (CPVI) combined with modified linear ablation (CPVI-MLA) vs. standalone CPVI in patients with long-standing persistent atrial fibrillation (LSPAF).
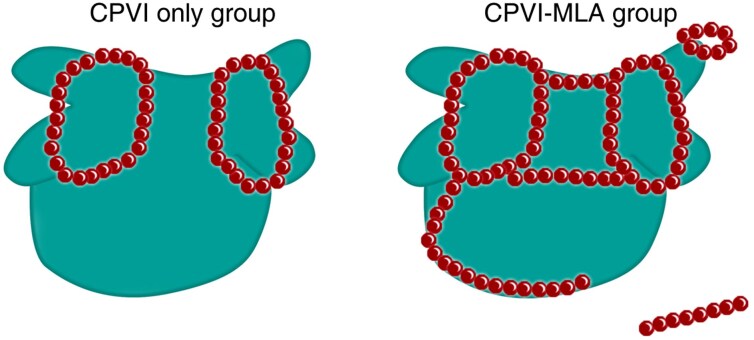
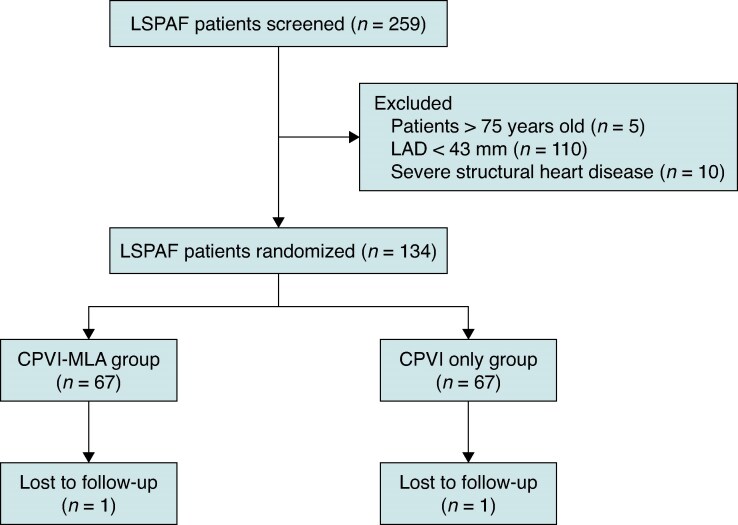
Methods and results: In this single-centre pilot trial, 134 LSPAF patients were randomized to the CPVI-MLA (n = 67) or CPVI-only (n = 67) groups. The CPVI-MLA protocol integrated four components: (i) ethanol infusion targeting the ligament of Marshall; (ii) complete CPVI; (iii) extended lesion sets (posterior wall isolation, dual isthmus ablation); and (iv) substrate modification [left atrial intima adjoining coronary sinus (LAI-CS) and superior vena cava isolation (SVCI)]. A 24 h Holter monitoring was performed at the 1st, 3rd, and 6th month follow-up visits, with 7-day Holter monitoring at the 12th month follow-up visit. The primary endpoint was freedom from atrial tachyarrhythmias (≥ 30 s) after the initial 3-month blanking period post-index procedure, without antiarrhythmic drugs. After a mean follow-up of 14.5 ± 9.1 months, 76.1% (51/67) in the CPVI-MLA group and 65.7% (44/67) in the CPVI-only group achieved the primary endpoint (P = 0.32). However, the CPVI-MLA group demonstrated significantly higher atrial fibrillation (AF)-free survival rate (91.0 vs. 76.1%, P = 0.049), while atrial tachycardia/atrial flutter-free survival rates were comparable (83.5 vs. 88.1%, P = 0.45). The CPVI-MLA strategy required longer ablation time (68.6 ± 12.3 vs. 49.4 ± 10.3 min, P < 0.001) and fluoroscopy exposure (14.9 ± 9.8 vs. 9.3 ± 6.7 min, P < 0.001). Serious adverse events were rare and similar between groups (1.5 vs. 0%, P = 1.00).
Conclusion: In patients with LSPAF, the CPVI-MLA strategy significantly improved freedom from AF compared with CPVI alone, although it did not improve overall sinus rhythm maintenance rate. This strategy may offer a refined approach for complex AF ablation, warranting further validation in larger trials.
期刊介绍:
EP - Europace - European Journal of Pacing, Arrhythmias and Cardiac Electrophysiology of the European Heart Rhythm Association of the European Society of Cardiology. The journal aims to provide an avenue of communication of top quality European and international original scientific work and reviews in the fields of Arrhythmias, Pacing and Cellular Electrophysiology. The Journal offers the reader a collection of contemporary original peer-reviewed papers, invited papers and editorial comments together with book reviews and correspondence.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


