Comparison of online adaptation strategies for magnetic resonance guided prostate radiation therapy
IF 3.3
Q2 ONCOLOGY
引用次数: 0
Abstract
Background and purpose
MR-guided adaptive radiation therapy allows for daily plan adaptation to account for anatomical changes. Two common strategies are adapt-to-position (ATP), involving re-optimization based on isocenter shifts, and adapt-to-shape (ATS), involving full recontouring and reoptimization. This study provides a dosimetric comparison of ATP and ATS using accumulated dose.
Materials and methods
Dose accumulation was performed for 35 patients with prostate cancer treated on a 1.5 T MR-Linac. All patients received ATS-based treatment with either 30.0 Gy in 5 fractions (30.0/5) or 42.7 Gy in 7 fractions (42.7/7), using a 5 mm isotropic PTV margin. ATP plans were retrospectively simulated. For each fraction, dose was mapped to a reference image using deformable image registration and summed across fractions. Fractional and accumulated dose-volume histogram (DVH) metrics were compared between ATS and ATP and correlated with daily anatomical variation.
Results
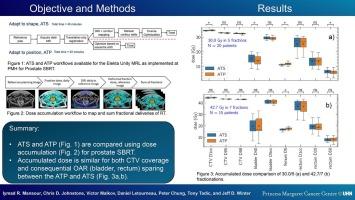
ATP and ATS achieved equivalent accumulated CTV D95 and D98 for both regimens. In the 30.0/5 cohort, small but statistically significant differences in OAR dose were observed: accumulated bladder D40 was 4 % lower for ATP (1.27 Gy; p = 0.0004), and rectum D50 was 1 % lower for ATP (0.40 Gy; p = 0.0008). Differences in rectum D1cc and bladder D5cc were not significant. In the 42.7/7 cohort, femur D5 was 3 % higher for ATP (0.83 Gy; p = 0.02); other differences were insignificant. Dosimetric differences across strategies correlated with interfraction motion.
Conclusion
ATP and ATS provided equivalent target coverage. OAR differences were statistically significant in some cases but remained within clinical tolerances, suggesting minimal clinical impact.
磁共振引导前列腺放射治疗在线适应策略比较
背景和目的磁共振引导的适应性放射治疗允许每日计划的调整,以解释解剖变化。两种常见的策略是适应位置(ATP),包括基于等中心位移的重新优化,以及适应形状(ATS),包括完全重新轮廓和重新优化。本研究采用累积剂量法对ATP和ATS进行剂量学比较。材料与方法对35例接受1.5 T MR-Linac治疗的前列腺癌患者进行剂量累积。所有患者均接受基于ats的治疗,采用5组30.0 Gy(30.0/5)或7组42.7 Gy(42.7/7),采用5 mm各向同性PTV切缘。对ATP计划进行回顾性模拟。对于每个分数,使用可变形图像配准将剂量映射到参考图像,并跨分数求和。比较ATS和ATP的分数和累积剂量-体积直方图(DVH)指标,并与每日解剖变化相关。结果两种治疗方案的累积CTV值D95和D98均相当。在30.0/5的队列中,观察到OAR剂量的微小但具有统计学意义的差异:ATP的膀胱累积D40降低了4% (1.27 Gy;p = 0.0004), ATP使直肠D50降低1% (0.40 Gy;p = 0.0008)。直肠D1cc和膀胱D5cc差异无统计学意义。在42.7/7组中,股骨D5因ATP升高3% (0.83 Gy;p = 0.02);其他差异不显著。不同策略的剂量学差异与干涉运动相关。结论atp与ATS的靶区覆盖相当。在一些病例中,OAR差异具有统计学意义,但仍在临床耐受范围内,表明临床影响很小。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文
来源期刊

Physics and Imaging in Radiation Oncology
Physics and Astronomy-Radiation
CiteScore
5.30
自引率
18.90%
发文量
93
审稿时长
6 weeks
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


