Clinician underprescription of and patient nonadherence to clinical practice guideline-recommended medications for peripheral artery disease: a systematic review and meta-analysis.
Aidan M Kirkham, Maude Paquet, Dean A Fergusson, Ian D Graham, Justin Presseau, Daniel I McIsaac, Sudhir K Nagpal, David de Launay, Sami Aftab Abdul, Risa Shorr, Jeremy M Grimshaw, Derek J Roberts
{"title":"Clinician underprescription of and patient nonadherence to clinical practice guideline-recommended medications for peripheral artery disease: a systematic review and meta-analysis.","authors":"Aidan M Kirkham, Maude Paquet, Dean A Fergusson, Ian D Graham, Justin Presseau, Daniel I McIsaac, Sudhir K Nagpal, David de Launay, Sami Aftab Abdul, Risa Shorr, Jeremy M Grimshaw, Derek J Roberts","doi":"10.1016/j.eclinm.2025.103391","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Guidelines recommend that adults with peripheral artery disease (PAD) take antiplatelets, statins, and antihypertensives. However, it is unclear how frequently clinicians do not prescribe these medications (ie, underprescription), how often patients fail to fill/refill their prescriptions (ie, nonadherence), which factors increase underprescription/nonadherence risk, and whether underprescription/nonadherence are associated with outcomes.</p><p><strong>Methods: </strong>We searched MEDLINE, EMBASE, CENTRAL, and Evidence-Based Medicine Reviews (January 1, 2006-to-February 18th, 2025) for studies reporting cumulative incidences/point prevalences of clinician underprescription and/or patient nonadherence to antiplatelets, statins, and/or antihypertensives; adjusted-risk factors for underprescription/nonadherence; and adjusted-outcomes associated with underprescription/nonadherence among adults with PAD. Two investigators independently screened citations, extracted data, and assessed risk of bias. Data were pooled using random-effects models. Estimate certainty was communicated using GRADE. The study was registered on PROSPERO (CRD42022362801).</p><p><strong>Findings: </strong>Among 4206 citations identified, 125 studies (n = 14,681,801 participants; 37% female) were included. The pooled cumulative incidence of antiplatelet, statin, and antihypertensive (among those with PAD and hypertension) underprescription was 28% (95% confidence interval [CI] = 21-36%; moderate-certainty), 34% (95% CI = 31-38%; high-certainty), and 43% (95% CI = 33-53%; moderate-certainty), respectively. The cumulative incidence of antiplatelet, statin, and antihypertensive nonadherence was 27% (95% CI = 20-35%; moderate-certainty), 28% (95% CI = 24-33%; high-certainty), and 23% (95% CI = 22-24%; low-certainty), respectively. Underprescription was more common in population-based studies and those enrolling more females and past/current smokers while nonadherence was more common in studies enrolling more patients with diabetes. Underprescription risk factors included female sex, advanced age, malignancy history, and chronic limb-threatening ischemia (all moderate-certainty). Nonadherence risk factors included advanced age, comorbidity burden, and receiving specialist mental health care (all moderate-certainty). Underprescription was associated with increased major adverse cardiac events, all-cause mortality, and decreased amputation-free time (all moderate-certainty).</p><p><strong>Interpretation: </strong>One-quarter-to-one-half of adults with PAD are not prescribed antiplatelets, statins, and antihypertensives. Further, approximately one-quarter of these patients do not adhere to these medications after prescription.</p><p><strong>Funding: </strong>This research was supported by a 2024 Vanier Canada Graduate Scholarship (awarded to AMK and supervised by DJR), a Graham Farquharson Physician Services Incorporated Knowledge Translation Fellowship (awarded to DJR), and a Research Program Award, University of OttawaDepartment of Surgery Annual Competition (awarded to DJR).</p>","PeriodicalId":11393,"journal":{"name":"EClinicalMedicine","volume":"86 ","pages":"103391"},"PeriodicalIF":10.0000,"publicationDate":"2025-07-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12337023/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"EClinicalMedicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.eclinm.2025.103391","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Guidelines recommend that adults with peripheral artery disease (PAD) take antiplatelets, statins, and antihypertensives. However, it is unclear how frequently clinicians do not prescribe these medications (ie, underprescription), how often patients fail to fill/refill their prescriptions (ie, nonadherence), which factors increase underprescription/nonadherence risk, and whether underprescription/nonadherence are associated with outcomes.
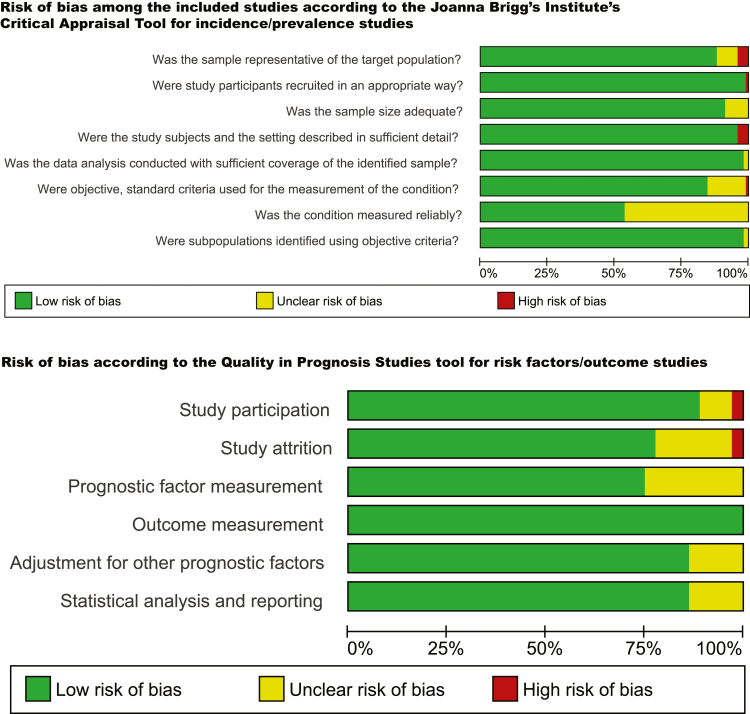
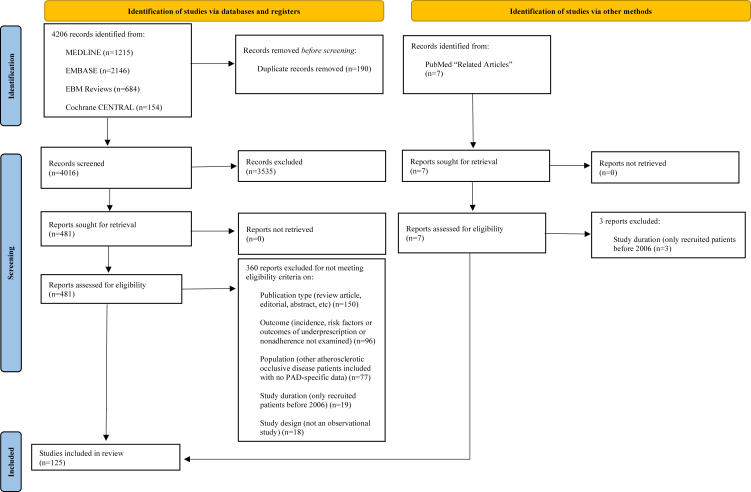
Methods: We searched MEDLINE, EMBASE, CENTRAL, and Evidence-Based Medicine Reviews (January 1, 2006-to-February 18th, 2025) for studies reporting cumulative incidences/point prevalences of clinician underprescription and/or patient nonadherence to antiplatelets, statins, and/or antihypertensives; adjusted-risk factors for underprescription/nonadherence; and adjusted-outcomes associated with underprescription/nonadherence among adults with PAD. Two investigators independently screened citations, extracted data, and assessed risk of bias. Data were pooled using random-effects models. Estimate certainty was communicated using GRADE. The study was registered on PROSPERO (CRD42022362801).
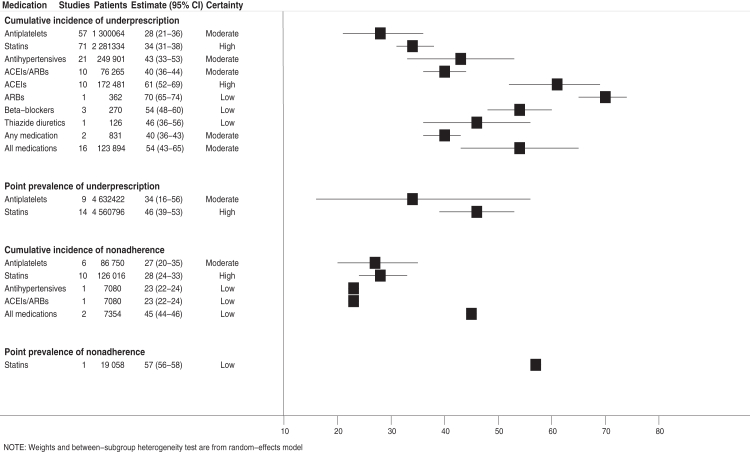
Findings: Among 4206 citations identified, 125 studies (n = 14,681,801 participants; 37% female) were included. The pooled cumulative incidence of antiplatelet, statin, and antihypertensive (among those with PAD and hypertension) underprescription was 28% (95% confidence interval [CI] = 21-36%; moderate-certainty), 34% (95% CI = 31-38%; high-certainty), and 43% (95% CI = 33-53%; moderate-certainty), respectively. The cumulative incidence of antiplatelet, statin, and antihypertensive nonadherence was 27% (95% CI = 20-35%; moderate-certainty), 28% (95% CI = 24-33%; high-certainty), and 23% (95% CI = 22-24%; low-certainty), respectively. Underprescription was more common in population-based studies and those enrolling more females and past/current smokers while nonadherence was more common in studies enrolling more patients with diabetes. Underprescription risk factors included female sex, advanced age, malignancy history, and chronic limb-threatening ischemia (all moderate-certainty). Nonadherence risk factors included advanced age, comorbidity burden, and receiving specialist mental health care (all moderate-certainty). Underprescription was associated with increased major adverse cardiac events, all-cause mortality, and decreased amputation-free time (all moderate-certainty).
Interpretation: One-quarter-to-one-half of adults with PAD are not prescribed antiplatelets, statins, and antihypertensives. Further, approximately one-quarter of these patients do not adhere to these medications after prescription.
Funding: This research was supported by a 2024 Vanier Canada Graduate Scholarship (awarded to AMK and supervised by DJR), a Graham Farquharson Physician Services Incorporated Knowledge Translation Fellowship (awarded to DJR), and a Research Program Award, University of OttawaDepartment of Surgery Annual Competition (awarded to DJR).
期刊介绍:
eClinicalMedicine is a gold open-access clinical journal designed to support frontline health professionals in addressing the complex and rapid health transitions affecting societies globally. The journal aims to assist practitioners in overcoming healthcare challenges across diverse communities, spanning diagnosis, treatment, prevention, and health promotion. Integrating disciplines from various specialties and life stages, it seeks to enhance health systems as fundamental institutions within societies. With a forward-thinking approach, eClinicalMedicine aims to redefine the future of healthcare.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


