{"title":"Rare coexistence of X-linked hyper immunoglobulin M syndrome and polyarticular juvenile idiopathic arthritis in a Chinese child: A case report.","authors":"Jing-Wei Li, Xue Xie, Xin-Yi Wei, Wei Zhang","doi":"10.52312/jdrs.2025.1988","DOIUrl":null,"url":null,"abstract":"<p><p>Immune dysregulation in children can lead to a variety of health issues, including infections, allergies and autoimmune diseases. However, the coexistence of autoimmune diseases and primary immunodeficiency disorders is extremely rare in clinical practice. A 4-year-old male patient was admitted in July 2017 with joint swelling and pain, alongside a history of recurrent respiratory infections and severe pneumonia. Physical examination revealed tenderness and swelling in multiple joints, and laboratory tests indicated elevated inflammatory markers. Imaging studies showed joint effusion and inflammatory lesions in the lungs. He was diagnosed with rheumatoid factor-negative polyarticular juvenile idiopathic arthritis (PJIA) and treatment was initiated with naproxen, methotrexate and etanercept, leading to significant symptom improvement. In July 2019, following a decline in immunoglobulin (Ig) M (IgM) levels (IgM 0.36 g/L) and recurrent infections, genetic testing was conducted, revealing a frameshift mutation in the CD40LG gene (c.621dup A, p.A208Sfs * 23), which confirmed the diagnosis of X-linked hyper IgM syndrome (XHIGM). The treatment regimen was adjusted to include monthly intravenous Ig infusions and prophylactic antibiotics, significantly reducing the frequency of respiratory infections. By January 2021, PJIA was in clinical remission, allowing for the discontinuation of immunosuppressive therapy, with follow-ups indicating continued recovery without discomfort. In conclusion, this case underscores the rare coexistence of XHIGM and PJIA in the field of pediatrics and identified a new pathogenic variant in CD40LG, enhancing our understanding of the clinical management of individuals with concurrent autoimmune and immunodeficiency disorders.</p>","PeriodicalId":73560,"journal":{"name":"Joint diseases and related surgery","volume":"36 3","pages":"751-756"},"PeriodicalIF":1.9000,"publicationDate":"2025-06-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12456349/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Joint diseases and related surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.52312/jdrs.2025.1988","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
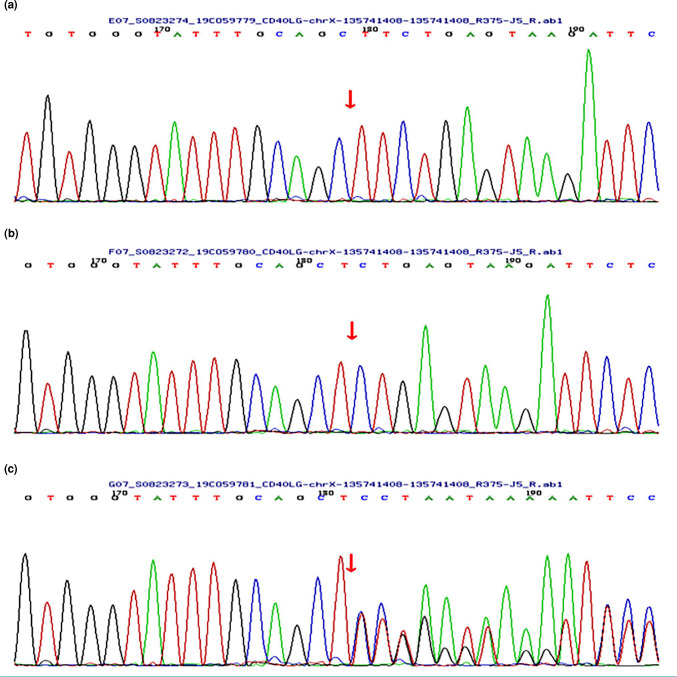
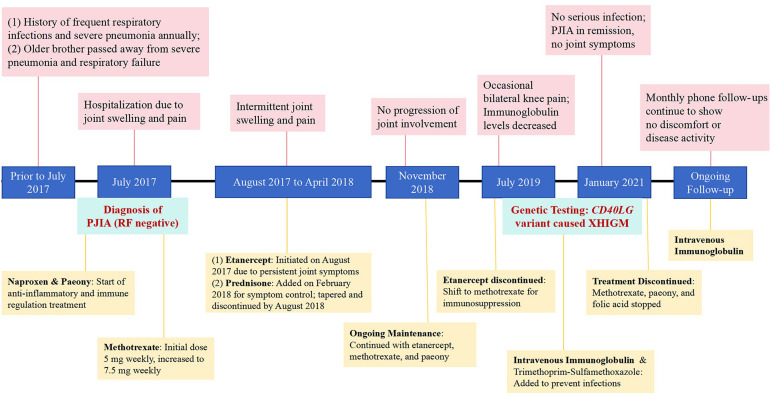
Immune dysregulation in children can lead to a variety of health issues, including infections, allergies and autoimmune diseases. However, the coexistence of autoimmune diseases and primary immunodeficiency disorders is extremely rare in clinical practice. A 4-year-old male patient was admitted in July 2017 with joint swelling and pain, alongside a history of recurrent respiratory infections and severe pneumonia. Physical examination revealed tenderness and swelling in multiple joints, and laboratory tests indicated elevated inflammatory markers. Imaging studies showed joint effusion and inflammatory lesions in the lungs. He was diagnosed with rheumatoid factor-negative polyarticular juvenile idiopathic arthritis (PJIA) and treatment was initiated with naproxen, methotrexate and etanercept, leading to significant symptom improvement. In July 2019, following a decline in immunoglobulin (Ig) M (IgM) levels (IgM 0.36 g/L) and recurrent infections, genetic testing was conducted, revealing a frameshift mutation in the CD40LG gene (c.621dup A, p.A208Sfs * 23), which confirmed the diagnosis of X-linked hyper IgM syndrome (XHIGM). The treatment regimen was adjusted to include monthly intravenous Ig infusions and prophylactic antibiotics, significantly reducing the frequency of respiratory infections. By January 2021, PJIA was in clinical remission, allowing for the discontinuation of immunosuppressive therapy, with follow-ups indicating continued recovery without discomfort. In conclusion, this case underscores the rare coexistence of XHIGM and PJIA in the field of pediatrics and identified a new pathogenic variant in CD40LG, enhancing our understanding of the clinical management of individuals with concurrent autoimmune and immunodeficiency disorders.
儿童免疫失调会导致各种健康问题,包括感染、过敏和自身免疫性疾病。然而,自身免疫性疾病与原发性免疫缺陷疾病共存在临床实践中极为罕见。一名4岁男性患者于2017年7月入院,伴有关节肿胀和疼痛,并有复发性呼吸道感染和严重肺炎史。体格检查显示多个关节有压痛和肿胀,实验室检查显示炎症标志物升高。影像学检查显示关节积液和肺部炎性病变。他被诊断为类风湿因子阴性多关节幼年特发性关节炎(PJIA),并开始使用萘普生、甲氨蝶呤和依那西普治疗,症状明显改善。2019年7月,在免疫球蛋白(Ig) M (IgM)水平下降(IgM 0.36 g/L)和反复感染后,进行基因检测,发现CD40LG基因(c.621dup a, p.A208Sfs * 23)发生移码突变,确诊为x连锁高IgM综合征(XHIGM)。调整治疗方案,包括每月静脉滴注Ig和预防性抗生素,显著降低呼吸道感染的频率。到2021年1月,PJIA处于临床缓解期,允许停止免疫抑制治疗,随访表明持续恢复无不适。总之,该病例强调了XHIGM和PJIA在儿科领域的罕见共存,并在CD40LG中发现了一种新的致病变异,增强了我们对并发自身免疫性和免疫缺陷疾病个体临床管理的理解。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


