{"title":"Influence of specific components of pericardial fat on coronary high-risk plaque prediction.","authors":"Lihong Nan, Tongli Li, Wenyu Ding, Mengshan Wu, Jintang Feng, Tianzhu Zhang, Fan Yang, Dong Li, Chunyang Sun, Ningnannan Zhang, Zhang Zhang","doi":"10.21037/qims-24-1140","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Coronary computed tomography angiography (CCTA) can be used to investigate the relationship between white adipose tissue (WAT) and brown adipose tissue (BAT) in pericardial fat (PF) and high-risk plaques (HRP) in patients with coronary artery disease (CAD). This study aimed to explore the association between specific components of PF and HRP/culprit ischemic plaques, as well as their mediating role in overall metabolic status, providing new imaging evidence for predicting adverse events in CAD.</p><p><strong>Methods: </strong>The clinical risk factors and imaging images of 107 CAD patients were retrospectively analyzed. Quantification of coronary artery calcium scores (CACS), PF, WAT, BAT, and pericardial fat attenuation (PFatt) were performed on non-contrast CT images. CCTA was used to evaluate myocardial ischemia and the presence of HRP. Fractional flow reserve derived from CCTA (CT-FFR) was performed in three major coronary arteries, with a threshold of ≤0.80 considered indicative of the presence of lesion-specific ischemia. HRP was defined as the presence of at least two of the four HRP features including positive remodeling (PR), low attenuation, napkin-ring sign (NRS), and spotty calcification. Mediator analysis was performed using Hayes (2018) Model-4.</p><p><strong>Results: </strong>A total of 107 CAD patients aged 65±8 years were included in this study. There were 49 patients (45.79%) with HRP and 57 patients (53.27%) with lesion-specific ischemia (CT-FFR ≤0.80). PF including WAT and BAT in the HRP group was significantly higher than that in the non-HRP group (PF: 241.28 <i>vs.</i> 204.94 cm<sup>3</sup>, P=0.005, WAT: 91.78 <i>vs.</i> 78.40 cm<sup>3</sup>, P=0.002, BAT: 56.25 <i>vs.</i> 46.71 cm<sup>3</sup>, P=0.008). Adding WAT to meaningful clinical risk factors and CACS increases the area under the curve (AUC) for HRP prediction {AUC [95% confidence interval (95% CI)]: 0.789 (0.692-0.887) <i>vs.</i> 0.655 (0.535-0.775), P<0.05}. Interestingly, adding PF to clinical risk factors and CACS decreased the AUC for the prediction of lesion-specific ischemia with no significant difference (P=0.083) [AUC (95% CI): 0.705 (0.592-0.817) <i>vs.</i> 0.796 (0.696-0.897), P<0.05]. Additionally, the mediation effect of PF accounted for 95.19% of the total effect of clinical risk factors on HRP (P<0.05).</p><p><strong>Conclusions: </strong>PF is associated with HRP, and clinical risk factors increase the risk of plaque rupture by promoting PF volume accumulation, especially WAT, which may be a potential predictor of HRP.</p>","PeriodicalId":54267,"journal":{"name":"Quantitative Imaging in Medicine and Surgery","volume":"15 8","pages":"7309-7322"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12332739/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Quantitative Imaging in Medicine and Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/qims-24-1140","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/29 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Coronary computed tomography angiography (CCTA) can be used to investigate the relationship between white adipose tissue (WAT) and brown adipose tissue (BAT) in pericardial fat (PF) and high-risk plaques (HRP) in patients with coronary artery disease (CAD). This study aimed to explore the association between specific components of PF and HRP/culprit ischemic plaques, as well as their mediating role in overall metabolic status, providing new imaging evidence for predicting adverse events in CAD.
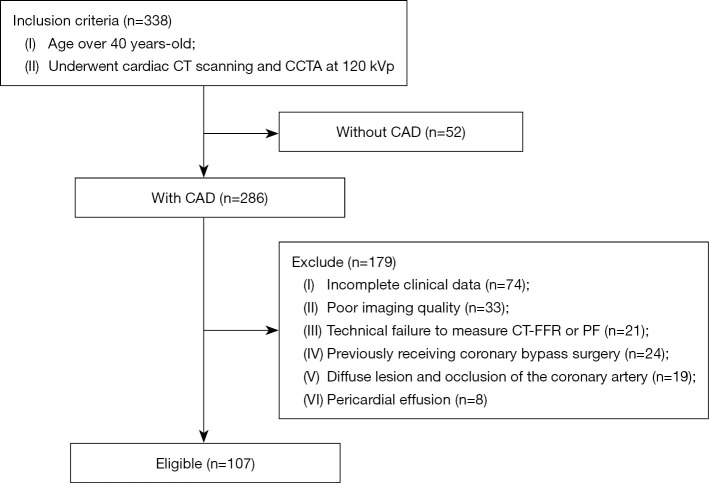
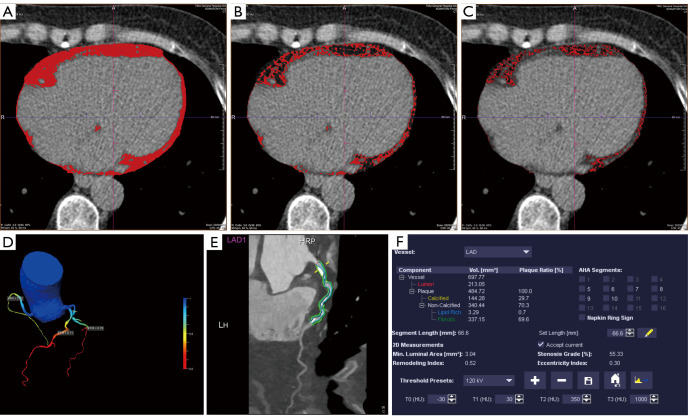
Methods: The clinical risk factors and imaging images of 107 CAD patients were retrospectively analyzed. Quantification of coronary artery calcium scores (CACS), PF, WAT, BAT, and pericardial fat attenuation (PFatt) were performed on non-contrast CT images. CCTA was used to evaluate myocardial ischemia and the presence of HRP. Fractional flow reserve derived from CCTA (CT-FFR) was performed in three major coronary arteries, with a threshold of ≤0.80 considered indicative of the presence of lesion-specific ischemia. HRP was defined as the presence of at least two of the four HRP features including positive remodeling (PR), low attenuation, napkin-ring sign (NRS), and spotty calcification. Mediator analysis was performed using Hayes (2018) Model-4.
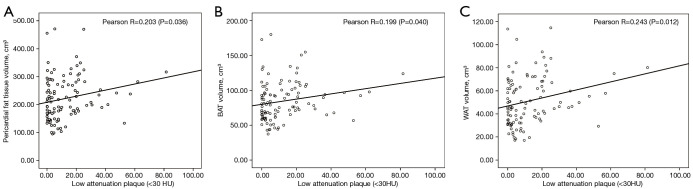
Results: A total of 107 CAD patients aged 65±8 years were included in this study. There were 49 patients (45.79%) with HRP and 57 patients (53.27%) with lesion-specific ischemia (CT-FFR ≤0.80). PF including WAT and BAT in the HRP group was significantly higher than that in the non-HRP group (PF: 241.28 vs. 204.94 cm3, P=0.005, WAT: 91.78 vs. 78.40 cm3, P=0.002, BAT: 56.25 vs. 46.71 cm3, P=0.008). Adding WAT to meaningful clinical risk factors and CACS increases the area under the curve (AUC) for HRP prediction {AUC [95% confidence interval (95% CI)]: 0.789 (0.692-0.887) vs. 0.655 (0.535-0.775), P<0.05}. Interestingly, adding PF to clinical risk factors and CACS decreased the AUC for the prediction of lesion-specific ischemia with no significant difference (P=0.083) [AUC (95% CI): 0.705 (0.592-0.817) vs. 0.796 (0.696-0.897), P<0.05]. Additionally, the mediation effect of PF accounted for 95.19% of the total effect of clinical risk factors on HRP (P<0.05).
Conclusions: PF is associated with HRP, and clinical risk factors increase the risk of plaque rupture by promoting PF volume accumulation, especially WAT, which may be a potential predictor of HRP.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


