Risk Factors for Correction Loss of Vertebral Slippage after Minimally Invasive Transforaminal Lumbar Interbody Fusion Surgery for Lumbar Degenerative Spondylolisthesis.
{"title":"Risk Factors for Correction Loss of Vertebral Slippage after Minimally Invasive Transforaminal Lumbar Interbody Fusion Surgery for Lumbar Degenerative Spondylolisthesis.","authors":"Yoshiaki Hiranaka, Shingo Miyazaki, Kohei Kuroshima, Masao Ryu, Shinichi Inoue, Takashi Yurube, Kenichiro Kakutani, Ko Tadokoro","doi":"10.22603/ssrr.2024-0285","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Some cases of postoperative correction loss have been observed in the reduction of vertebral slippage using a percutaneous pedicle screw system for lumbar degenerative spondylolisthesis. We aimed to identify the risk factors for correction loss after minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) and to determine the effect of postoperative correction loss on postoperative clinical outcomes.</p><p><strong>Methods: </strong>In this retrospective study, a total of 111 patients (mean age 69.5 years, 37 men and 74 women) who underwent single-level MIS-TLIF with slippage reduction for lumbar degenerative spondylolisthesis and were followed up for >1 year were included in the study. The correction loss group (group L) included those with a correction loss of ≥3 mm between immediately after surgery and 1 year after surgery, and the correction maintenance group (group M) included those with a correction loss <3 mm. Demographic data, preoperative and postoperative radiographic measurements, and clinical outcomes were collected, and the risk factors in group L and clinical outcomes in the two groups were analyzed statistically.</p><p><strong>Results: </strong>Groups L and M comprised 19 and 92 cases, respectively. High pelvic incidence-lumbar lordosis (odds ratio [OR]: 1.16, 95% confidence interval [CI]: 1.07-1.25, p<0.001), high slip vertebra slope (OR: 1.22, 95% CI: 1.07-1.39, p<0.001), and ≥10° segmental angulation (OR: 15.00, 95% CI: 3.04-73.95, p=0.0022) were risk factors for correction loss; however, low bone density was not. The Oswestry Disability Index and Visual Analog Scale scores for low back pain, leg pain, and leg numbness were not significantly different between both groups; however, the bone union rate at 6 months postoperatively was significantly lower in group L (p=0.0020).</p><p><strong>Conclusions: </strong>Postoperative correction loss was influenced by preoperative sagittal alignment and instability rather than bone density. Patients with correction loss tend to have prolonged bone union and should be closely monitored.</p>","PeriodicalId":22253,"journal":{"name":"Spine Surgery and Related Research","volume":"9 4","pages":"443-452"},"PeriodicalIF":1.2000,"publicationDate":"2025-02-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12330377/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine Surgery and Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22603/ssrr.2024-0285","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/27 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Some cases of postoperative correction loss have been observed in the reduction of vertebral slippage using a percutaneous pedicle screw system for lumbar degenerative spondylolisthesis. We aimed to identify the risk factors for correction loss after minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) and to determine the effect of postoperative correction loss on postoperative clinical outcomes.
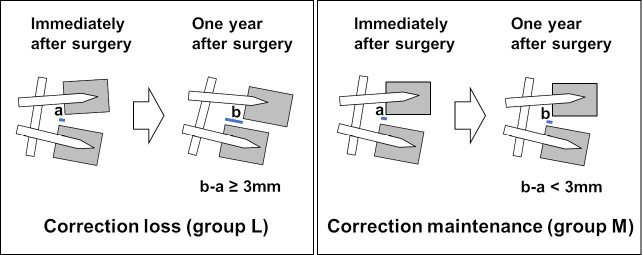
Methods: In this retrospective study, a total of 111 patients (mean age 69.5 years, 37 men and 74 women) who underwent single-level MIS-TLIF with slippage reduction for lumbar degenerative spondylolisthesis and were followed up for >1 year were included in the study. The correction loss group (group L) included those with a correction loss of ≥3 mm between immediately after surgery and 1 year after surgery, and the correction maintenance group (group M) included those with a correction loss <3 mm. Demographic data, preoperative and postoperative radiographic measurements, and clinical outcomes were collected, and the risk factors in group L and clinical outcomes in the two groups were analyzed statistically.
Results: Groups L and M comprised 19 and 92 cases, respectively. High pelvic incidence-lumbar lordosis (odds ratio [OR]: 1.16, 95% confidence interval [CI]: 1.07-1.25, p<0.001), high slip vertebra slope (OR: 1.22, 95% CI: 1.07-1.39, p<0.001), and ≥10° segmental angulation (OR: 15.00, 95% CI: 3.04-73.95, p=0.0022) were risk factors for correction loss; however, low bone density was not. The Oswestry Disability Index and Visual Analog Scale scores for low back pain, leg pain, and leg numbness were not significantly different between both groups; however, the bone union rate at 6 months postoperatively was significantly lower in group L (p=0.0020).
Conclusions: Postoperative correction loss was influenced by preoperative sagittal alignment and instability rather than bone density. Patients with correction loss tend to have prolonged bone union and should be closely monitored.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


