Cost per Response of Acthar® Gel vs Standard of Care for the Treatment of Proteinuria in Nephrotic Syndrome Due to Idiopathic Membranous Nephropathy Among Adults from the US Healthcare Perspective.
Jas Bindra, Ishveen Chopra, Kyle Hayes, John Niewoehner, Mary P Panaccio, George J Wan
{"title":"Cost per Response of Acthar® Gel vs Standard of Care for the Treatment of Proteinuria in Nephrotic Syndrome Due to Idiopathic Membranous Nephropathy Among Adults from the US Healthcare Perspective.","authors":"Jas Bindra, Ishveen Chopra, Kyle Hayes, John Niewoehner, Mary P Panaccio, George J Wan","doi":"10.36469/001c.142078","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Proteinuria, a critical marker of glomerulosclerosis, poses a challenge in idiopathic membranous nephropathy (iMN), particularly when standard treatments fail. Acthar® Gel, a US Food and Drug Administration-approved treatment option, may offer an alternative for managing refractory proteinuria in nephrotic syndrome (NS) due to iMN where multiple treatments have failed. <b>Objective:</b> The cost per response of Acthar® Gel vs standard of care (SoC; cyclophosphamide or rituximab) for treatment of proteinuria in NS due to iMN was evaluated among adults who had failed multiple treatments from a US payer perspective over a 1- to 3-year horizon. <b>Methods:</b> A probabilistic, cohort-level state-transition model simulated patient progression through various health states using 6-month cycles. Patients began in a relapse phase and received either Acthar® Gel or SoC. Transition probabilities determined whether patients achieved a response, experienced no response, progressed to renal failure, or remained in relapse. Responders could potentially maintain their response or relapse, while nonresponders risked renal failure, with potential mortality from any state. Clinical, healthcare resource utilization, and cost data were derived from published literature. Drug prices were based on wholesale acquisition costs. <b>Results:</b> Over 1 year, Acthar® Gel showed a lower cost per response ( <math><mn>377</mn> <mrow><mo> </mo></mrow> <mn>185</mn> <mo>)</mo> <mi>t</mi> <mi>h</mi> <mi>a</mi> <mi>n</mi> <mi>c</mi> <mi>y</mi> <mi>c</mi> <mi>l</mi> <mi>o</mi> <mi>p</mi> <mi>h</mi> <mi>o</mi> <mi>s</mi> <mi>p</mi> <mi>h</mi> <mi>a</mi> <mi>m</mi> <mi>i</mi> <mi>d</mi> <mi>e</mi> <mo>(</mo></math> 551 687) and rituximab ($741 373). This cost advantage of Acthar® Gel was maintained over 2 and 3 years. Acthar® Gel had higher drug acquisition costs than cyclophosphamide and rituximab but resulted in lower overall medical costs and higher response rates within 1 year, without additional treatment-related costs. Over 2 and 3 years, Acthar® Gel had a lower overall cost of care and higher response rates than SoC, establishing it as a dominant treatment option. <b>Conclusions:</b> Based on current model assumptions and clinical inputs, Acthar® Gel may potentially be a cost-effective and value-based treatment strategy vs unapproved SoCs for adults with refractory proteinuria in NS due to iMN, particularly for those who have not responded to conventional therapies over a 1- to 3-year period within a US payer context. These results may inform clinical and payer decision-making in cases when other standard therapies fail to achieve desired outcomes for a specific population.</p>","PeriodicalId":16012,"journal":{"name":"Journal of Health Economics and Outcomes Research","volume":"12 2","pages":"50-61"},"PeriodicalIF":2.3000,"publicationDate":"2025-08-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12333935/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Health Economics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36469/001c.142078","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
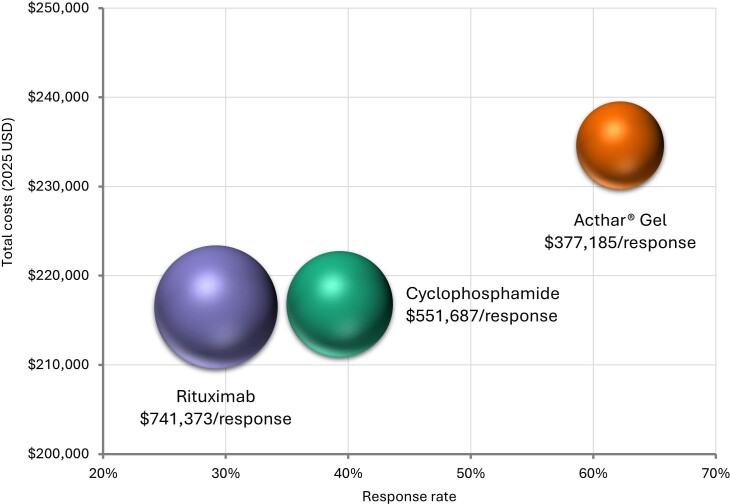
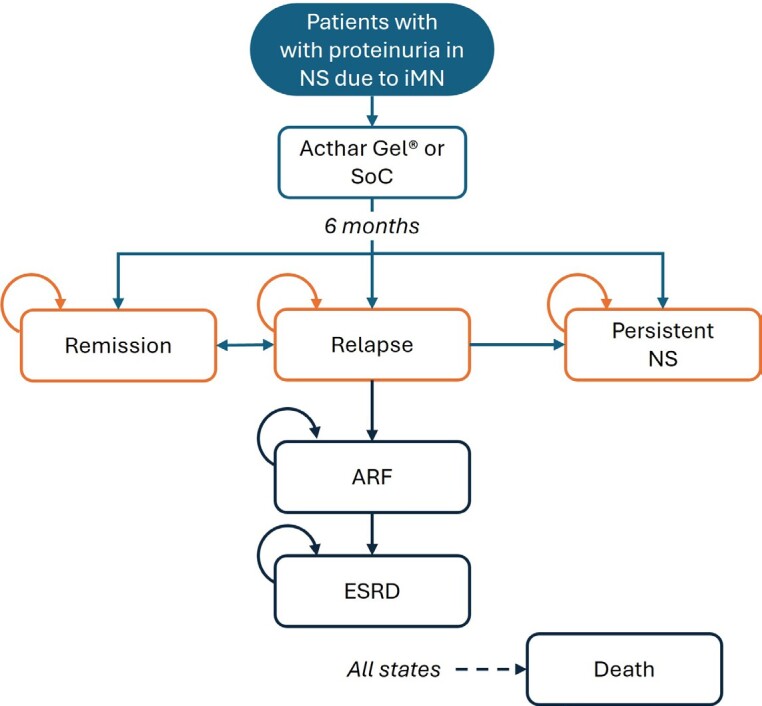
Background: Proteinuria, a critical marker of glomerulosclerosis, poses a challenge in idiopathic membranous nephropathy (iMN), particularly when standard treatments fail. Acthar® Gel, a US Food and Drug Administration-approved treatment option, may offer an alternative for managing refractory proteinuria in nephrotic syndrome (NS) due to iMN where multiple treatments have failed. Objective: The cost per response of Acthar® Gel vs standard of care (SoC; cyclophosphamide or rituximab) for treatment of proteinuria in NS due to iMN was evaluated among adults who had failed multiple treatments from a US payer perspective over a 1- to 3-year horizon. Methods: A probabilistic, cohort-level state-transition model simulated patient progression through various health states using 6-month cycles. Patients began in a relapse phase and received either Acthar® Gel or SoC. Transition probabilities determined whether patients achieved a response, experienced no response, progressed to renal failure, or remained in relapse. Responders could potentially maintain their response or relapse, while nonresponders risked renal failure, with potential mortality from any state. Clinical, healthcare resource utilization, and cost data were derived from published literature. Drug prices were based on wholesale acquisition costs. Results: Over 1 year, Acthar® Gel showed a lower cost per response ( 551 687) and rituximab ($741 373). This cost advantage of Acthar® Gel was maintained over 2 and 3 years. Acthar® Gel had higher drug acquisition costs than cyclophosphamide and rituximab but resulted in lower overall medical costs and higher response rates within 1 year, without additional treatment-related costs. Over 2 and 3 years, Acthar® Gel had a lower overall cost of care and higher response rates than SoC, establishing it as a dominant treatment option. Conclusions: Based on current model assumptions and clinical inputs, Acthar® Gel may potentially be a cost-effective and value-based treatment strategy vs unapproved SoCs for adults with refractory proteinuria in NS due to iMN, particularly for those who have not responded to conventional therapies over a 1- to 3-year period within a US payer context. These results may inform clinical and payer decision-making in cases when other standard therapies fail to achieve desired outcomes for a specific population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


