{"title":"From Fluttering Hearts to Restless Stomach: Navigating Atrial Fibrillation, Ablation and Gastroparesis.","authors":"Rabia Riasat, Anas Atrash","doi":"10.12890/2025_005596","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We present a case of severe gastroparesis with pyloric spasm secondary to radiofrequency catheter ablation (RFCA) with a focus on procedural risk factors, prevention, and treatment modalities.</p><p><strong>Case report: </strong>A 39-year-old man with paroxysmal atrial fibrillation underwent RFCA after failed pharmaceutical treatment. The procedure involved three-dimensional mapping and controlled RFCA near the oesophagus. Post-procedure, he developed severe abdominal pain, distention, and vomiting. Imaging revealed stomach distention and pyloric spasm. An upper endoscopy confirmed gastroparesis due to ablation. Metoclopramide was administered, improving food tolerance. However, persistent symptoms led to a gastric emptying study showing delayed emptying, consistent with gastroparesis. Despite treatment with metoclopramide, the patient's symptoms persisted, prompting consideration of esophageal botulinum toxin and medication changes for symptom management.</p><p><strong>Conclusions: </strong>In a patient with no prior history of abdominal symptoms or chronic gastric disorder post ablation presentation of new-onset abdominal distention, pain, and vomiting ablation-induced gastroparesis should be high on the differential and different treatment modalities should be tried if severe symptoms such as postprandial regurgitation persist. Moreover, better oesophageal protection strategies should be implemented, and guidelines be added to procedure performance limiting excessive force, energy, manipulation, and introduction of oesophageal temperature control holding parameters.</p><p><strong>Learning points: </strong>Gastroparesis can be an under-recognized complication of left atrial ablation.Posterior wall ablation near the oesophagus is high-risk for gastrointestinal complications.Symptoms usually persist for 3-6 months but may last long term.</p>","PeriodicalId":11908,"journal":{"name":"European journal of case reports in internal medicine","volume":"12 8","pages":"005596"},"PeriodicalIF":0.0000,"publicationDate":"2025-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12331283/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European journal of case reports in internal medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12890/2025_005596","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: We present a case of severe gastroparesis with pyloric spasm secondary to radiofrequency catheter ablation (RFCA) with a focus on procedural risk factors, prevention, and treatment modalities.
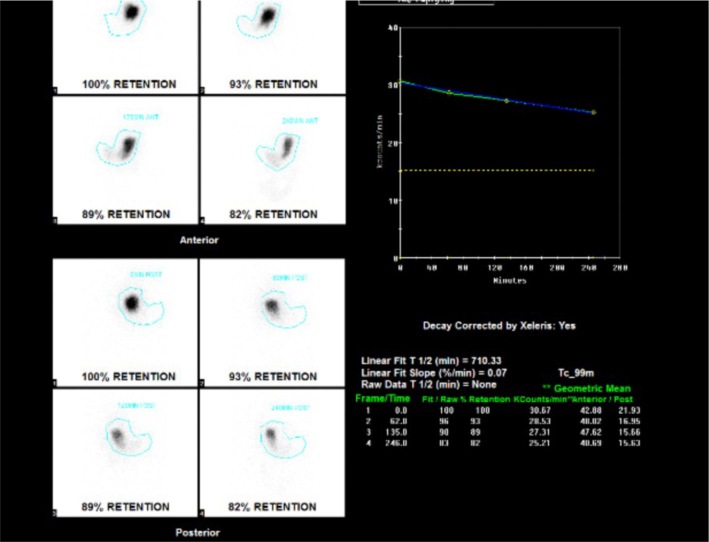
Case report: A 39-year-old man with paroxysmal atrial fibrillation underwent RFCA after failed pharmaceutical treatment. The procedure involved three-dimensional mapping and controlled RFCA near the oesophagus. Post-procedure, he developed severe abdominal pain, distention, and vomiting. Imaging revealed stomach distention and pyloric spasm. An upper endoscopy confirmed gastroparesis due to ablation. Metoclopramide was administered, improving food tolerance. However, persistent symptoms led to a gastric emptying study showing delayed emptying, consistent with gastroparesis. Despite treatment with metoclopramide, the patient's symptoms persisted, prompting consideration of esophageal botulinum toxin and medication changes for symptom management.
Conclusions: In a patient with no prior history of abdominal symptoms or chronic gastric disorder post ablation presentation of new-onset abdominal distention, pain, and vomiting ablation-induced gastroparesis should be high on the differential and different treatment modalities should be tried if severe symptoms such as postprandial regurgitation persist. Moreover, better oesophageal protection strategies should be implemented, and guidelines be added to procedure performance limiting excessive force, energy, manipulation, and introduction of oesophageal temperature control holding parameters.
Learning points: Gastroparesis can be an under-recognized complication of left atrial ablation.Posterior wall ablation near the oesophagus is high-risk for gastrointestinal complications.Symptoms usually persist for 3-6 months but may last long term.
期刊介绍:
The European Journal of Case Reports in Internal Medicine is an official journal of the European Federation of Internal Medicine (EFIM), representing 35 national societies from 33 European countries. The Journal''s mission is to promote the best medical practice and innovation in the field of acute and general medicine. It also provides a forum for internal medicine doctors where they can share new approaches with the aim of improving diagnostic and clinical skills in this field. EJCRIM welcomes high-quality case reports describing unusual or complex cases that an internist may encounter in everyday practice. The cases should either demonstrate the appropriateness of a diagnostic/therapeutic approach, describe a new procedure or maneuver, or show unusual manifestations of a disease or unexpected reactions. The Journal only accepts and publishes those case reports whose learning points provide new insight and/or contribute to advancing medical knowledge both in terms of diagnostics and therapeutic approaches. Case reports of medical errors, therefore, are also welcome as long as they provide innovative measures on how to prevent them in the current practice (Instructive Errors). The Journal may also consider brief and reasoned reports on issues relevant to the practice of Internal Medicine, as well as Abstracts submitted to the scientific meetings of acknowledged medical societies.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


