C M Kensen, Lisa Wiersema, Anja Betgen, Doenja M J Lambregts, Corrie A M Marijnen, Uulke A van der Heide, Tomas M Janssen
{"title":"From standardized to individualized margins for online adaptive tumor dose escalation in rectal cancer.","authors":"C M Kensen, Lisa Wiersema, Anja Betgen, Doenja M J Lambregts, Corrie A M Marijnen, Uulke A van der Heide, Tomas M Janssen","doi":"10.1186/s13014-025-02706-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To determine the impact of tumor characteristics such as tumor volume, circumference and location in the rectum on intrafraction motion during dose-escalated MRI-guided radiotherapy of rectal cancer and to explore the potential of PTV margin individualization.</p><p><strong>Methods: </strong>Seventy-seven rectal cancer patients, treated with short course radiotherapy (SCRT) on a 1.5T MR-Linac, were included in the study. For all five treatment fractions per patient, the GTV of the primary tumor was manually delineated on T2-weighted images acquired for online plan adaptation (MRI<sub>adapt</sub>). GTV delineations on the MRI acquired for verification after irradiation (MRI<sub>post</sub>) were obtained by patient-specific fine-tuning of a population-based GTV autosegmentation model using the delineation on MRI<sub>adapt</sub>. The intrafraction motion was calculated as ¾ of the center of gravity (COG) displacement of the GTV between MRI<sub>adapt</sub> and MRI<sub>post</sub>. PTV margins were calculated using the Van Herk recipe. The effect of tumor volume, circumference and location in the rectum on intrafraction motion was studied using linear mixed effect modeling and individualized margins were calculated for each group.</p><p><strong>Results: </strong>Intrafraction motion was correlated with tumor location with larger displacement in Anterior-Posterior (p = 0.001) and Cranial-Caudal (CC; p = 0.043) direction for caudal tumors compared to proximal tumors (lower border starting > 5 cm from anorectal junction). For tumor volume, a significant (p = 0.049), but small association with Left-Right motion was found, with larger tumors exhibiting larger motion. PTV margins required for the full cohort were 2.8 mm LR, 6.3 mm AP, 2.2 mm cranial and 5.6 mm caudal. Individualizing on tumor location resulted in AP margin of 3.5 mm for proximal rectal tumors and 6.7 mm for distal rectal tumors. Margins in CC direction were 3.2 mm for proximal rectal tumors and asymmetrically 2.0 mm cranial and 6.0 mm caudal for distal rectal tumors.</p><p><strong>Conclusion: </strong>Our study demonstrated that distance to anorectal junction significantly influenced the magnitude and direction of the intrafraction motion of rectal cancer patients receiving SCRT, with distal tumors showing larger motion in the AP and CC directions. For proximal rectal tumors, the margin could be decreased in AP and CC direction.</p>","PeriodicalId":49639,"journal":{"name":"Radiation Oncology","volume":"20 1","pages":"125"},"PeriodicalIF":3.3000,"publicationDate":"2025-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12335123/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13014-025-02706-8","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To determine the impact of tumor characteristics such as tumor volume, circumference and location in the rectum on intrafraction motion during dose-escalated MRI-guided radiotherapy of rectal cancer and to explore the potential of PTV margin individualization.
Methods: Seventy-seven rectal cancer patients, treated with short course radiotherapy (SCRT) on a 1.5T MR-Linac, were included in the study. For all five treatment fractions per patient, the GTV of the primary tumor was manually delineated on T2-weighted images acquired for online plan adaptation (MRIadapt). GTV delineations on the MRI acquired for verification after irradiation (MRIpost) were obtained by patient-specific fine-tuning of a population-based GTV autosegmentation model using the delineation on MRIadapt. The intrafraction motion was calculated as ¾ of the center of gravity (COG) displacement of the GTV between MRIadapt and MRIpost. PTV margins were calculated using the Van Herk recipe. The effect of tumor volume, circumference and location in the rectum on intrafraction motion was studied using linear mixed effect modeling and individualized margins were calculated for each group.
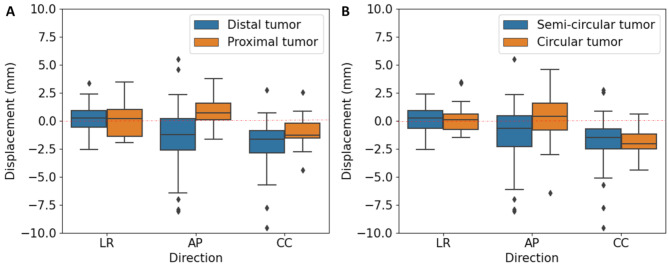
Results: Intrafraction motion was correlated with tumor location with larger displacement in Anterior-Posterior (p = 0.001) and Cranial-Caudal (CC; p = 0.043) direction for caudal tumors compared to proximal tumors (lower border starting > 5 cm from anorectal junction). For tumor volume, a significant (p = 0.049), but small association with Left-Right motion was found, with larger tumors exhibiting larger motion. PTV margins required for the full cohort were 2.8 mm LR, 6.3 mm AP, 2.2 mm cranial and 5.6 mm caudal. Individualizing on tumor location resulted in AP margin of 3.5 mm for proximal rectal tumors and 6.7 mm for distal rectal tumors. Margins in CC direction were 3.2 mm for proximal rectal tumors and asymmetrically 2.0 mm cranial and 6.0 mm caudal for distal rectal tumors.
Conclusion: Our study demonstrated that distance to anorectal junction significantly influenced the magnitude and direction of the intrafraction motion of rectal cancer patients receiving SCRT, with distal tumors showing larger motion in the AP and CC directions. For proximal rectal tumors, the margin could be decreased in AP and CC direction.
Radiation OncologyONCOLOGY-RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING
CiteScore
6.50
自引率
2.80%
发文量
181
审稿时长
3-6 weeks
期刊介绍:
Radiation Oncology encompasses all aspects of research that impacts on the treatment of cancer using radiation. It publishes findings in molecular and cellular radiation biology, radiation physics, radiation technology, and clinical oncology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


