Ifael Yerosias Mauleti, Krishna Adi Wibisana, Djati Prasetio Syamsuridzal, Sri Mulyati, Vivi Lisdawati, Harimat Hendarwan, Ika Saptarini
{"title":"Rapid Antiretroviral Therapy Initiation Reduces Mortality Among People Living With HIV in Indonesia: A Retrospective Observational Study.","authors":"Ifael Yerosias Mauleti, Krishna Adi Wibisana, Djati Prasetio Syamsuridzal, Sri Mulyati, Vivi Lisdawati, Harimat Hendarwan, Ika Saptarini","doi":"10.3961/jpmph.24.622","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Current recommendations for managing human immunodeficiency virus (HIV) propose that initiating antiretroviral therapy (ART) promptly after diagnosis, regardless of CD4 cell count, may decrease illness and mortality risk. This study aimed to investigate factors associated with reduced mortality, including the time to ART initiation after diagnosis with HIV.</p><p><strong>Methods: </strong>We conducted a retrospective cohort study using the medical records of 326 people living with human immunodeficiency virus (PLHIV) aged 18 years or older who initiated ART at a tertiary hospital between January 2018 and December 2022. We employed Cox regression models to estimate survival and identify mortality predictors, considering variables with p-values less than 0.05 as statistically significant.</p><p><strong>Results: </strong>From 2018 to 2022, 19.9% of PLHIV initiated ART within 7 days of diagnosis, and 57 participants died. The final multivariable Cox proportional hazards model indicated that earlier ART initiation significantly reduced mortality risk compared with starting ART more than 60 days after diagnosis, with adjusted hazard ratios of 0.36 for initiation within 7 days and 0.42 for initiation between 8 days and 60 days. Additional characteristics associated with reduced mortality risk included a CD4 count above 200 cells/mm 3 before ART initiation, a lower World Health Organization clinical stage, and tuberculosis post-exposure prophylaxis.</p><p><strong>Conclusions: </strong>Earlier ART initiation significantly lowered mortality rates. Furthermore, a pre-ART CD4 count above 200 cells/mm3, a lower clinical stage, and tuberculosis preventive therapy were associated with reduced mortality risk among PLHIV. Future studies should investigate additional predictors of mortality within a prospective cohort study framework.</p>","PeriodicalId":520687,"journal":{"name":"Journal of preventive medicine and public health = Yebang Uihakhoe chi","volume":"58 4","pages":"360-369"},"PeriodicalIF":2.1000,"publicationDate":"2025-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12332387/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of preventive medicine and public health = Yebang Uihakhoe chi","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3961/jpmph.24.622","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/22 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Current recommendations for managing human immunodeficiency virus (HIV) propose that initiating antiretroviral therapy (ART) promptly after diagnosis, regardless of CD4 cell count, may decrease illness and mortality risk. This study aimed to investigate factors associated with reduced mortality, including the time to ART initiation after diagnosis with HIV.
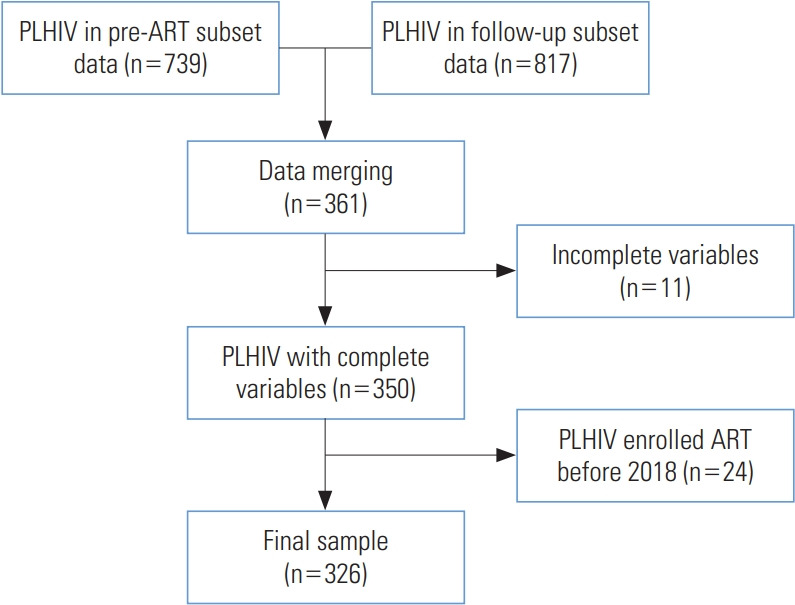
Methods: We conducted a retrospective cohort study using the medical records of 326 people living with human immunodeficiency virus (PLHIV) aged 18 years or older who initiated ART at a tertiary hospital between January 2018 and December 2022. We employed Cox regression models to estimate survival and identify mortality predictors, considering variables with p-values less than 0.05 as statistically significant.
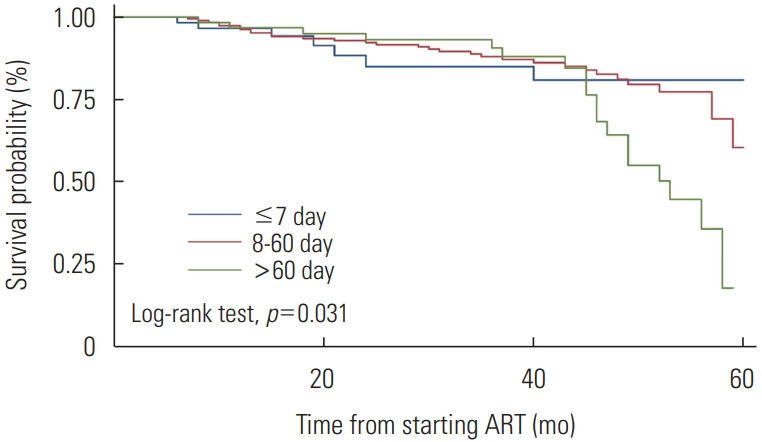
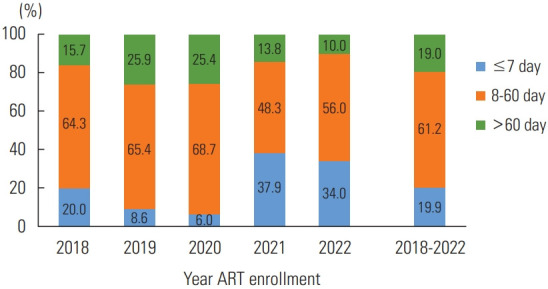
Results: From 2018 to 2022, 19.9% of PLHIV initiated ART within 7 days of diagnosis, and 57 participants died. The final multivariable Cox proportional hazards model indicated that earlier ART initiation significantly reduced mortality risk compared with starting ART more than 60 days after diagnosis, with adjusted hazard ratios of 0.36 for initiation within 7 days and 0.42 for initiation between 8 days and 60 days. Additional characteristics associated with reduced mortality risk included a CD4 count above 200 cells/mm 3 before ART initiation, a lower World Health Organization clinical stage, and tuberculosis post-exposure prophylaxis.
Conclusions: Earlier ART initiation significantly lowered mortality rates. Furthermore, a pre-ART CD4 count above 200 cells/mm3, a lower clinical stage, and tuberculosis preventive therapy were associated with reduced mortality risk among PLHIV. Future studies should investigate additional predictors of mortality within a prospective cohort study framework.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


