{"title":"Frailty and comorbidity in COVID-19 patients with and without ICU admission restrictions: a retrospective observational study.","authors":"Felix Starlander, Erland Östberg","doi":"10.1186/s44158-025-00268-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Limited resources during the COVID-19 pandemic made ICU admission decisions ethically complex. In Sweden, where ICU bed availability per capita is among the lowest in Europe, clinical judgment guided triage decisions, as prognostic scoring systems like the Clinical Frailty Scale (CFS) and Age-adjusted Charlson Comorbidity Index (ACCI) were not routinely used. This study aimed to compare patients considered eligible for intensive care with those for whom ICU admission was restricted and to evaluate whether a post hoc assessment of frailty and comorbidity aligned with clinical decision making.</p><p><strong>Methods: </strong>This retrospective observational study included 204 COVID-19-positive patients admitted to a Swedish secondary hospital during the first pandemic wave. Patients were categorized as either eligible for intensive care (ICU group) or having a documented ICU admission restriction (ICU restriction group). Electronic medical records were reviewed to assign CFS and ACCI scores, and a combined score was calculated to better reflect overall frailty and comorbidity burden.</p><p><strong>Results: </strong>The ICU group had a mean age of 68 years versus 83 years in the ICU restriction group. Of the ICU group, 26 out of 100 patients (26%) were ultimately admitted to intensive care. Median combined CFS + ACCI scores were 5 (IQR 5-6) in the ICU group and 12 (IQR 11-14) in the ICU restriction group; difference in score: 7 (95% CI, 6-8; p < 0.001). The combined score demonstrated clear separation between the groups with minimal overlap: in the ICU group, 95% of patients had a combined score below 8.3, while in the ICU restriction group, 95% of patients had a score above 8.4.</p><p><strong>Conclusions: </strong>Marked contrasts in age, frailty, and comorbidity burden distinguished patients eligible for intensive care from those with an ICU admission restriction, reflecting a close correspondence between the prognostic scoring systems and clinical judgment. Integrating the CFS and ACCI into a single combined score sharpened the analysis and may prove useful in future research or as a triage tool, although further validation of this approach is warranted.</p>","PeriodicalId":73597,"journal":{"name":"Journal of Anesthesia, Analgesia and Critical Care (Online)","volume":"5 1","pages":"51"},"PeriodicalIF":3.1000,"publicationDate":"2025-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12333239/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Anesthesia, Analgesia and Critical Care (Online)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44158-025-00268-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Limited resources during the COVID-19 pandemic made ICU admission decisions ethically complex. In Sweden, where ICU bed availability per capita is among the lowest in Europe, clinical judgment guided triage decisions, as prognostic scoring systems like the Clinical Frailty Scale (CFS) and Age-adjusted Charlson Comorbidity Index (ACCI) were not routinely used. This study aimed to compare patients considered eligible for intensive care with those for whom ICU admission was restricted and to evaluate whether a post hoc assessment of frailty and comorbidity aligned with clinical decision making.
Methods: This retrospective observational study included 204 COVID-19-positive patients admitted to a Swedish secondary hospital during the first pandemic wave. Patients were categorized as either eligible for intensive care (ICU group) or having a documented ICU admission restriction (ICU restriction group). Electronic medical records were reviewed to assign CFS and ACCI scores, and a combined score was calculated to better reflect overall frailty and comorbidity burden.
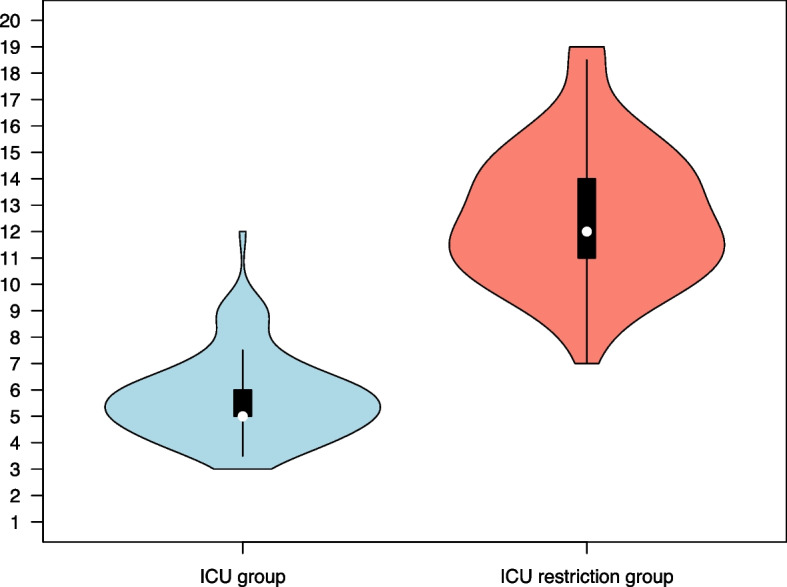
Results: The ICU group had a mean age of 68 years versus 83 years in the ICU restriction group. Of the ICU group, 26 out of 100 patients (26%) were ultimately admitted to intensive care. Median combined CFS + ACCI scores were 5 (IQR 5-6) in the ICU group and 12 (IQR 11-14) in the ICU restriction group; difference in score: 7 (95% CI, 6-8; p < 0.001). The combined score demonstrated clear separation between the groups with minimal overlap: in the ICU group, 95% of patients had a combined score below 8.3, while in the ICU restriction group, 95% of patients had a score above 8.4.
Conclusions: Marked contrasts in age, frailty, and comorbidity burden distinguished patients eligible for intensive care from those with an ICU admission restriction, reflecting a close correspondence between the prognostic scoring systems and clinical judgment. Integrating the CFS and ACCI into a single combined score sharpened the analysis and may prove useful in future research or as a triage tool, although further validation of this approach is warranted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


