Rory F L Hammond, Nikhil Manoj, Anna Bridgens, Fergal Monsell, Abhinav Singh, Yael Gelfer
{"title":"Paediatric type I open tibia fractures: are antibiotics alone sufficient?","authors":"Rory F L Hammond, Nikhil Manoj, Anna Bridgens, Fergal Monsell, Abhinav Singh, Yael Gelfer","doi":"10.1302/2633-1462.68.BJO-2025-0060.R1","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The conventional management of the soft-tissue component of an open fracture involves emergent debridement. There is, however, evidence that questions this approach in the management of Gustilo-Anderson type I open fractures in paediatric patients. This systematic review aims to explore differences in infection rates between nonoperative management with antibiotics and operative debridement in children with type I open lower limb tibial fractures that do not require surgical fixation.</p><p><strong>Methods: </strong>A systematic review following the PRISMA guidelines was conducted. Patients aged under 18 years with Gustilo-Anderson type I open tibia fractures treated with either antibiotics alone or operative debridement were included. Polytrauma patients and those requiring operative fracture stabilization were excluded. Study bias was assessed with the ROBINS-I (Risk of Bias in Non-randomized Studies of Interventions) tool.</p><p><strong>Results: </strong>Ten retrospective studies of 123 patients with Gustilo-Anderson type I open tibial fractures were included. Nonoperative management in the emergency department with antibiotics was used in 41 patients, with two infections reported (4.87%). Operative debridement was performed in 82 patients, with two infections reported (2.33%).</p><p><strong>Conclusion: </strong>The optimum management for paediatric Gustilo-Anderson type I open tibia fractures remains unclear. There may be selected cases, with true low-energy injury without operative fixation requirements, which can be managed in the emergency department. However, there is not sufficient high-quality evidence to advocate for regular deviation from current guidelines in open tibia fractures in paediatric patients. Decision-making must take into account the energy absorbed, as this factor can be misleading within the current classification system.</p>","PeriodicalId":34103,"journal":{"name":"Bone & Joint Open","volume":"6 8","pages":"905-914"},"PeriodicalIF":3.1000,"publicationDate":"2025-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12331384/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bone & Joint Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1302/2633-1462.68.BJO-2025-0060.R1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: The conventional management of the soft-tissue component of an open fracture involves emergent debridement. There is, however, evidence that questions this approach in the management of Gustilo-Anderson type I open fractures in paediatric patients. This systematic review aims to explore differences in infection rates between nonoperative management with antibiotics and operative debridement in children with type I open lower limb tibial fractures that do not require surgical fixation.
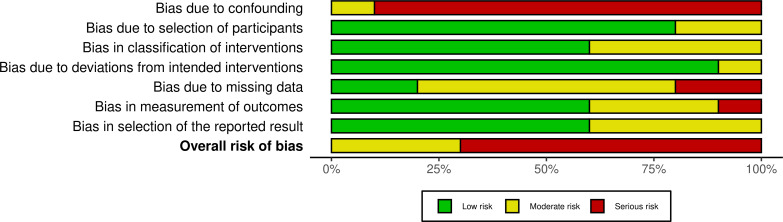
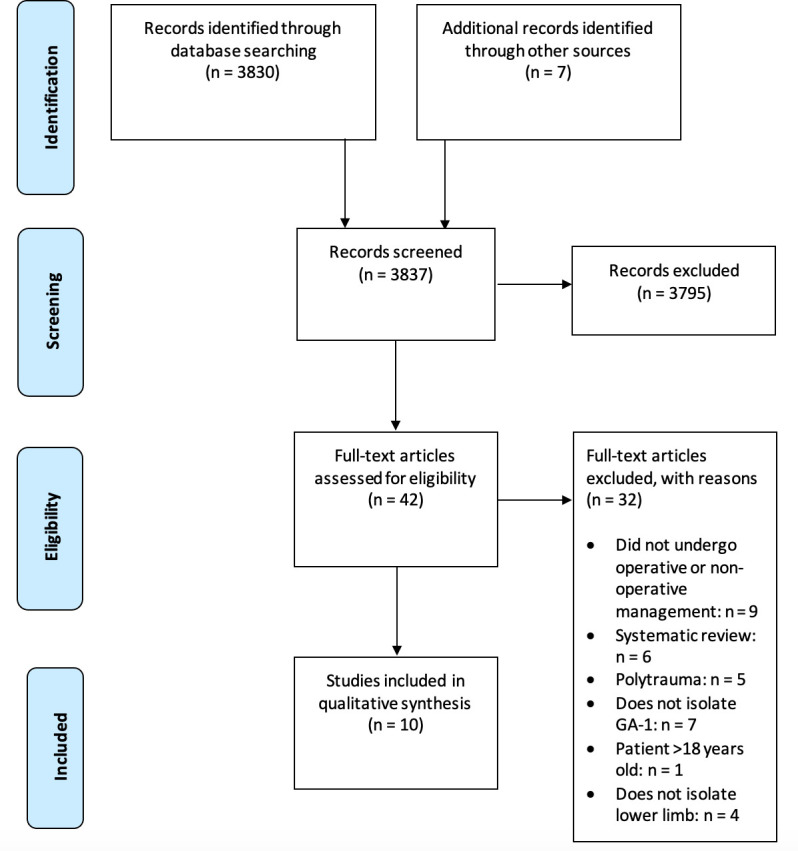
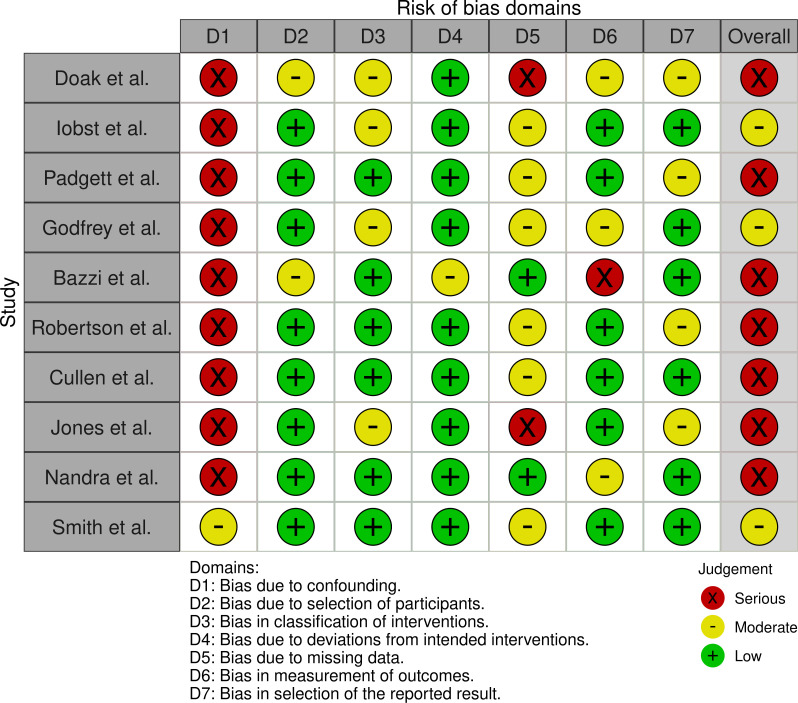
Methods: A systematic review following the PRISMA guidelines was conducted. Patients aged under 18 years with Gustilo-Anderson type I open tibia fractures treated with either antibiotics alone or operative debridement were included. Polytrauma patients and those requiring operative fracture stabilization were excluded. Study bias was assessed with the ROBINS-I (Risk of Bias in Non-randomized Studies of Interventions) tool.
Results: Ten retrospective studies of 123 patients with Gustilo-Anderson type I open tibial fractures were included. Nonoperative management in the emergency department with antibiotics was used in 41 patients, with two infections reported (4.87%). Operative debridement was performed in 82 patients, with two infections reported (2.33%).
Conclusion: The optimum management for paediatric Gustilo-Anderson type I open tibia fractures remains unclear. There may be selected cases, with true low-energy injury without operative fixation requirements, which can be managed in the emergency department. However, there is not sufficient high-quality evidence to advocate for regular deviation from current guidelines in open tibia fractures in paediatric patients. Decision-making must take into account the energy absorbed, as this factor can be misleading within the current classification system.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


