Development and Validation of a Nomogram to Predict Ventricular Fibrillation During Percutaneous Coronary Intervention in Patients With Acute Myocardial Infarction.
{"title":"Development and Validation of a Nomogram to Predict Ventricular Fibrillation During Percutaneous Coronary Intervention in Patients With Acute Myocardial Infarction.","authors":"Ruifeng Liu, Xiangyu Gao, Jihong Fan, Huiqiang Zhao","doi":"10.31083/RCM37301","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Ventricular fibrillation (VF) is a life-threatening complication of acute myocardial infarction (AMI), particularly in patients undergoing percutaneous coronary intervention (PCI). Early identification of high-risk patients is crucial for implementing preventive measures and improving outcomes.</p><p><strong>Methods: </strong>This retrospective study analyzed clinical, laboratory, and angiographic data from 155 AMI patients to identify predictors of VF during PCI. Variable selection was performed using least absolute shrinkage and selection operator (LASSO) regression, elastic net regression, and random forest. Independent predictors were identified through multivariable logistic regression, and a nomogram was developed and validated to predict VF risk. Model performance was assessed using receiver operating characteristic (ROC) and calibration curves.</p><p><strong>Results: </strong>Independent predictors of VF included diabetes (OR = 3.676 (1.365-10.668); <i>p</i> = 0.012), neutrophil-to-lymphocyte ratio (NLR) (odds ratio (OR) = 1.149 (1.053-1.265); <i>p</i> = 0.002), right coronary artery (RCA) intervention (OR = 3.185 (1.088-9.804); <i>p</i> = 0.037), Gensini score (OR = 1.020 (1.007-1.033); <i>p</i> = 0.003), and absence of beta blockers (OR = 0.168 (0.054-0.472); <i>p</i> = 0.001). The nomogram, incorporating these predictors, demonstrated a strong discriminative ability with an area under the ROC curve (AUC) of 0.882 (0.825-0.939) and good calibration (Hosmer-Lemeshow test, <i>p</i> = 0.769). The calibration curve showed a strong alignment between predicted probabilities and observed outcomes, with a mean absolute error of 0.033.</p><p><strong>Conclusions: </strong>This study identified diabetes, NLR, RCA intervention, Gensini score, and absence of beta-blocker use as key predictors of VF during PCI in AMI patients. A nomogram incorporating these factors showed strong predictive performance, aiding clinicians in identifying high-risk patients for targeted preventive strategies.</p>","PeriodicalId":20989,"journal":{"name":"Reviews in cardiovascular medicine","volume":"26 7","pages":"37301"},"PeriodicalIF":1.3000,"publicationDate":"2025-07-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12326412/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reviews in cardiovascular medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.31083/RCM37301","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Ventricular fibrillation (VF) is a life-threatening complication of acute myocardial infarction (AMI), particularly in patients undergoing percutaneous coronary intervention (PCI). Early identification of high-risk patients is crucial for implementing preventive measures and improving outcomes.
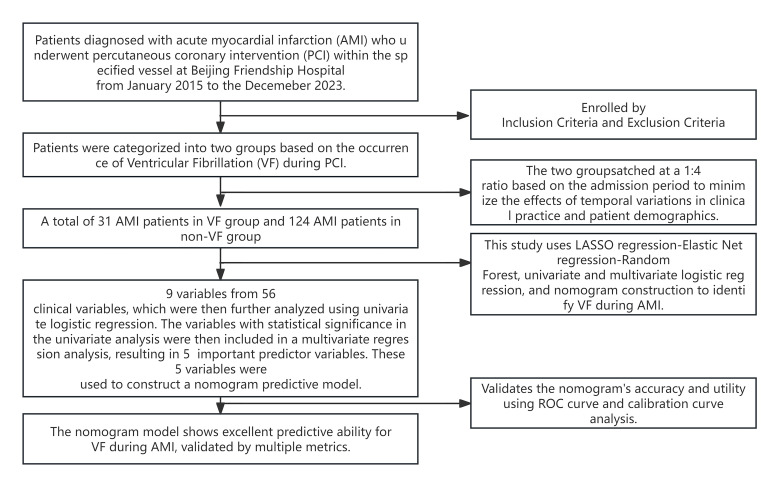
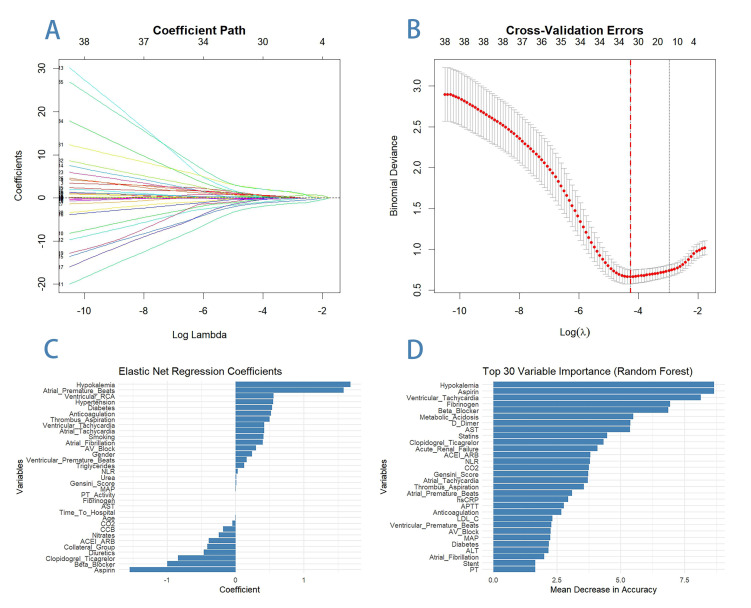
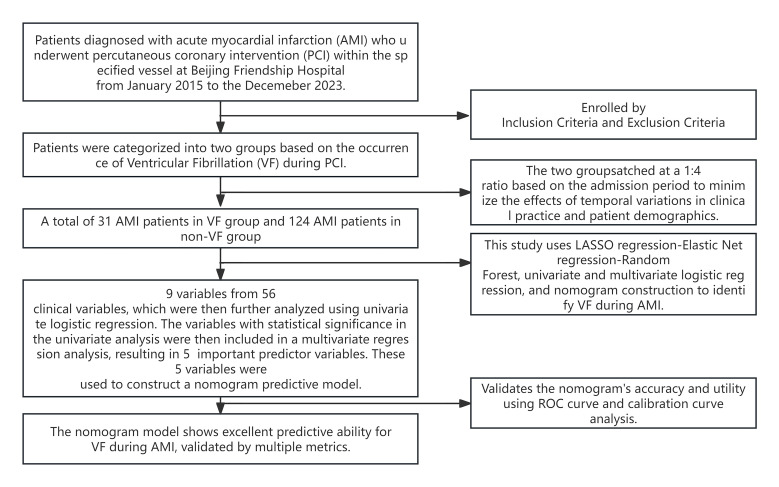
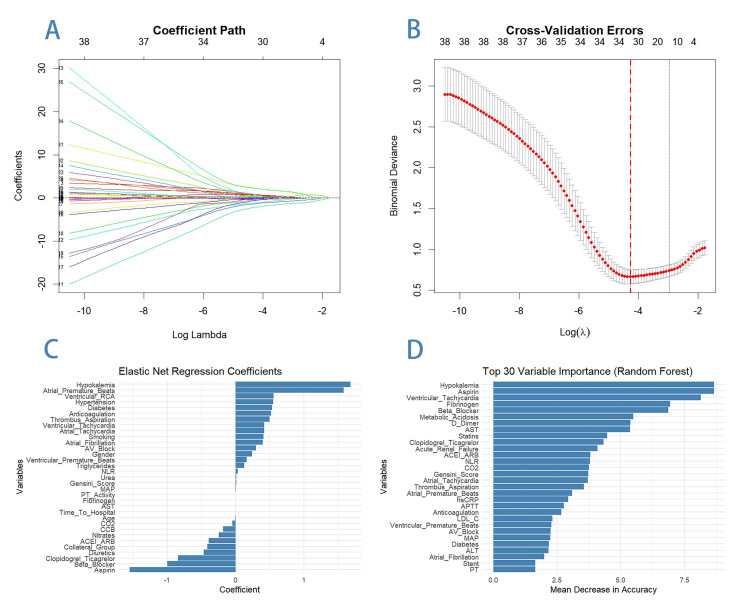
Methods: This retrospective study analyzed clinical, laboratory, and angiographic data from 155 AMI patients to identify predictors of VF during PCI. Variable selection was performed using least absolute shrinkage and selection operator (LASSO) regression, elastic net regression, and random forest. Independent predictors were identified through multivariable logistic regression, and a nomogram was developed and validated to predict VF risk. Model performance was assessed using receiver operating characteristic (ROC) and calibration curves.
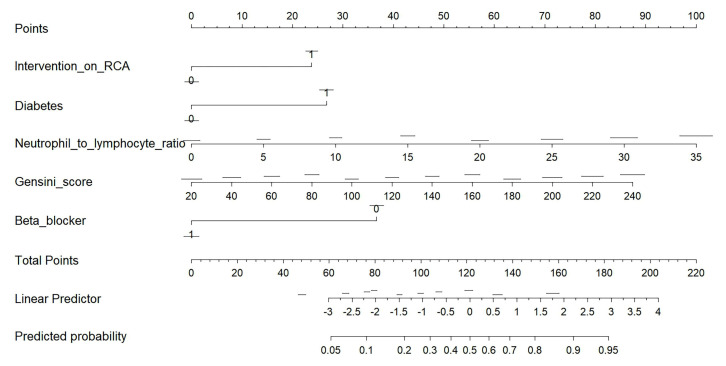
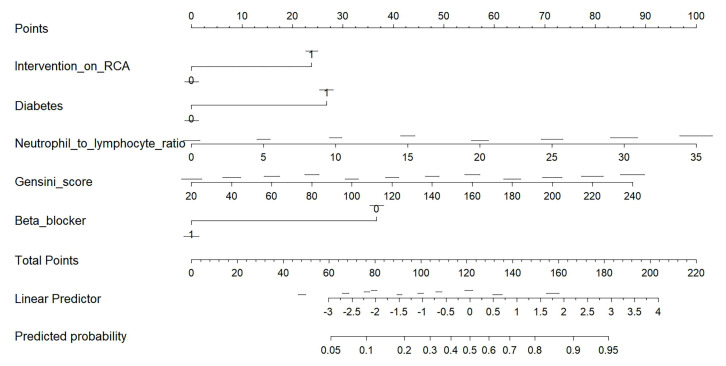
Results: Independent predictors of VF included diabetes (OR = 3.676 (1.365-10.668); p = 0.012), neutrophil-to-lymphocyte ratio (NLR) (odds ratio (OR) = 1.149 (1.053-1.265); p = 0.002), right coronary artery (RCA) intervention (OR = 3.185 (1.088-9.804); p = 0.037), Gensini score (OR = 1.020 (1.007-1.033); p = 0.003), and absence of beta blockers (OR = 0.168 (0.054-0.472); p = 0.001). The nomogram, incorporating these predictors, demonstrated a strong discriminative ability with an area under the ROC curve (AUC) of 0.882 (0.825-0.939) and good calibration (Hosmer-Lemeshow test, p = 0.769). The calibration curve showed a strong alignment between predicted probabilities and observed outcomes, with a mean absolute error of 0.033.
Conclusions: This study identified diabetes, NLR, RCA intervention, Gensini score, and absence of beta-blocker use as key predictors of VF during PCI in AMI patients. A nomogram incorporating these factors showed strong predictive performance, aiding clinicians in identifying high-risk patients for targeted preventive strategies.
期刊介绍:
RCM is an international, peer-reviewed, open access journal. RCM publishes research articles, review papers and short communications on cardiovascular medicine as well as research on cardiovascular disease. We aim to provide a forum for publishing papers which explore the pathogenesis and promote the progression of cardiac and vascular diseases. We also seek to establish an interdisciplinary platform, focusing on translational issues, to facilitate the advancement of research, clinical treatment and diagnostic procedures. Heart surgery, cardiovascular imaging, risk factors and various clinical cardiac & vascular research will be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


