{"title":"Access to Limited Critical Care and Risk of Mortality in Rwanda: A Prospective Cohort Study.","authors":"Alex Mezei, Donatien Hitayezu, Tyler Gilman, Jeffrey Bone, Celestin Hategaka, Srinivas Murthy, Marla McKnight, Theogene Twagirumugabe","doi":"10.1097/CCE.0000000000001298","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>There is a large discrepancy between need and access to critical care in low- and middle-income countries. Little is known about what subgroups of patients are being prioritized for critical care.</p><p><strong>Objectives: </strong>The primary objective was to assess what clinical, demographic, and socioeconomic variables were associated with timely ICU admission. Secondary objectives included determining the rate of ICU admission among patients who met admission criteria, inpatient mortality, and length of stay.</p><p><strong>Design: </strong>Prospective cohort study.</p><p><strong>Setting and participants: </strong>All adult patients meeting ICU admission criteria at the University Teaching Hospital of Butare, Huye, Rwanda.</p><p><strong>Main outcomes and measures: </strong>The primary outcome was the proportion of patients admitted to ICU within 24 hours of being identified as critically ill. A multivariable logistic regression model was used to assess whether clinical, demographic, or socioeconomic factors are associated with timely ICU admission. Secondary outcomes were the proportion of patients admitted to ICU at any time, inpatient mortality, and length of stay.</p><p><strong>Results: </strong>Three hundred eighteen patients were enrolled between January 24, 2024, and June 3, 2024. Eighty-eight (27.7%) were admitted to ICU within 24 hours. Requiring ICU for postoperative recovery (odds ratio [OR], 8.21; 95% CI, 3.64-19.8), obstetric patients (OR, 2.43; 95% CI, 0.92-6.41), and ICU bed availability (OR, 1.26; 95% CI, 1.02-1.55) increased the odds of timely ICU admission in multivariable analysis. Socioeconomic status, gender, and social connections had minimal association with ICU admission, with wide CIs. The inpatient mortality rate was 44.0% and average length of stay was 14 days.</p><p><strong>Conclusions and relevance: </strong>Obstetric and postoperative patients are prioritized for ICU admission. There is a large unmet need for critical care in Rwanda, and mortality among critically ill patients is high.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 8","pages":"e1298"},"PeriodicalIF":2.7000,"publicationDate":"2025-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12333700/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001298","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: There is a large discrepancy between need and access to critical care in low- and middle-income countries. Little is known about what subgroups of patients are being prioritized for critical care.
Objectives: The primary objective was to assess what clinical, demographic, and socioeconomic variables were associated with timely ICU admission. Secondary objectives included determining the rate of ICU admission among patients who met admission criteria, inpatient mortality, and length of stay.
Design: Prospective cohort study.
Setting and participants: All adult patients meeting ICU admission criteria at the University Teaching Hospital of Butare, Huye, Rwanda.
Main outcomes and measures: The primary outcome was the proportion of patients admitted to ICU within 24 hours of being identified as critically ill. A multivariable logistic regression model was used to assess whether clinical, demographic, or socioeconomic factors are associated with timely ICU admission. Secondary outcomes were the proportion of patients admitted to ICU at any time, inpatient mortality, and length of stay.
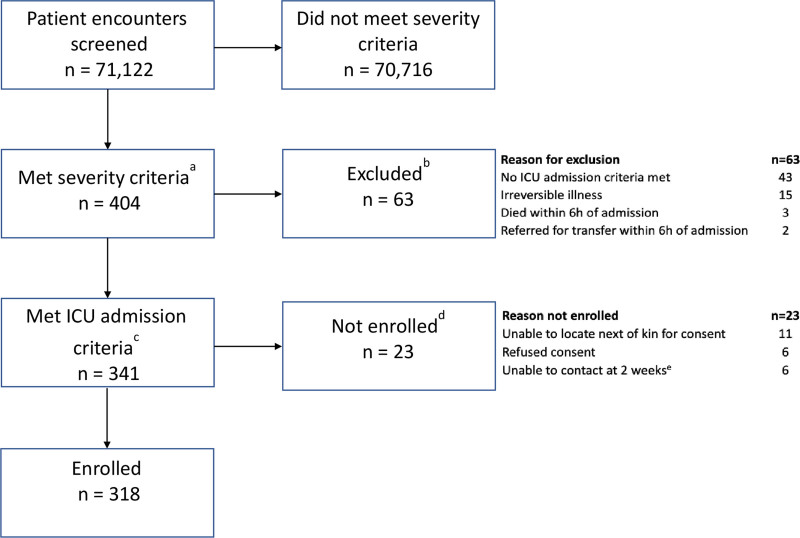
Results: Three hundred eighteen patients were enrolled between January 24, 2024, and June 3, 2024. Eighty-eight (27.7%) were admitted to ICU within 24 hours. Requiring ICU for postoperative recovery (odds ratio [OR], 8.21; 95% CI, 3.64-19.8), obstetric patients (OR, 2.43; 95% CI, 0.92-6.41), and ICU bed availability (OR, 1.26; 95% CI, 1.02-1.55) increased the odds of timely ICU admission in multivariable analysis. Socioeconomic status, gender, and social connections had minimal association with ICU admission, with wide CIs. The inpatient mortality rate was 44.0% and average length of stay was 14 days.
Conclusions and relevance: Obstetric and postoperative patients are prioritized for ICU admission. There is a large unmet need for critical care in Rwanda, and mortality among critically ill patients is high.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


