A Machine Learning-Based Prognostication Model Enhances Prediction of Early Hepatic Encephalopathy in Patients With Noncancer-Related Cirrhosis: Multicenter Longitudinal Cohort Study in Taiwan.
{"title":"A Machine Learning-Based Prognostication Model Enhances Prediction of Early Hepatic Encephalopathy in Patients With Noncancer-Related Cirrhosis: Multicenter Longitudinal Cohort Study in Taiwan.","authors":"Hsin-Yu Chen, Yiu-Hua Cheng, Wei-Chung Yeh, Yi-Chuan Chen, Yi-Wen Tsai","doi":"10.2196/71229","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hepatic encephalopathy (HE) contributes significantly to mortality among patients with liver cirrhosis. Early prediction of HE is essential for clinical decision-making, yet remains challenging-particularly in noncancer-related cirrhosis due to the unpredictable disease course.</p><p><strong>Objective: </strong>This study aimed to develop a novel machine learning (ML) model to improve early prediction of HE in patients with noncancer-related cirrhosis.</p><p><strong>Methods: </strong>A multicenter, retrospective cohort study was conducted from January 2010 to December 2017 across all Chang Gung Memorial Hospital branches in northern, middle, and southern Taiwan. We applied several ML models to evaluate HE predictability and compared their performance in the training dataset and testing dataset. Optimal sensitivity and specificity were determined using the Youden index. The best ML model was interpreted by the Shapley Additive Explanations plot.</p><p><strong>Results: </strong>A total of 5878 patients with cirrhosis were included in the analysis, of whom 1187 (20.2%) subsequently developed HE. Compared to the non-HE group, patients with HE were older (median age 55, IQR 46-65 vs median age 54, IQR 44-66 years; P=.04) and had higher rates of hepatitis B virus infection (351/1187, 30% vs 961/4691, 20.5%; P<.001), alcohol use (540/1187, 45.5% vs 1512/4691, 32.2%; P<.001), sepsis (393/1187, 33.1% vs 792/4691, 16.9%; P<.001), and mortality (425/1187, 35.8% vs 502/4691, 10.7%; P<.001), along with distinct laboratory abnormalities reflecting liver dysfunction. Among the ML algorithms evaluated, the extreme gradient boosting algorithm demonstrated the highest predictive accuracy, achieving an area under the curve (AUC) of 0.86 (95% CI 0.83-0.88) in the testing dataset. This performance was significantly superior to that of the neural network (AUC 0.79, 95% CI 0.76-0.81; P<.001), support vector machine (AUC 0.77, 95% CI 0.73-0.80; P<.001), and the model for end-stage liver disease score (AUC 0.74, 95% CI 0.71-0.77; P<.001). Using a probability threshold of 0.25, the extreme gradient boosting model demonstrated a sensitivity of 72% (95% CI 0.67-0.77), specificity of 80% (95% CI 0.78-0.82), a positive predictive value of 48% (95% CI 43-53), and a negative predictive value of 92% (95% CI 90-94) in the testing set. Comparable performance was observed in the training dataset, with a sensitivity of 80% (95% CI 0.77-0.83), specificity of 81% (95% CI 0.80-0.82), and a negative predictive value of 94% at the same threshold. The most influential predictive variables identified by the model included serum ammonia, aspartate transaminase, alanine transaminase, prothrombin time, and serum potassium.</p><p><strong>Conclusions: </strong>We developed a novel ML model for predicting HE in patients with noncancer-related cirrhosis. This model provides a practical guide to help physicians and these patients in shared decision-making regarding treatment strategy, with the ultimate goal of improving clinical care and reducing the burden of HE-related morbid complications.</p>","PeriodicalId":56334,"journal":{"name":"JMIR Medical Informatics","volume":"13 ","pages":"e71229"},"PeriodicalIF":3.8000,"publicationDate":"2025-08-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12327908/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Medical Informatics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2196/71229","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICAL INFORMATICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Hepatic encephalopathy (HE) contributes significantly to mortality among patients with liver cirrhosis. Early prediction of HE is essential for clinical decision-making, yet remains challenging-particularly in noncancer-related cirrhosis due to the unpredictable disease course.
Objective: This study aimed to develop a novel machine learning (ML) model to improve early prediction of HE in patients with noncancer-related cirrhosis.
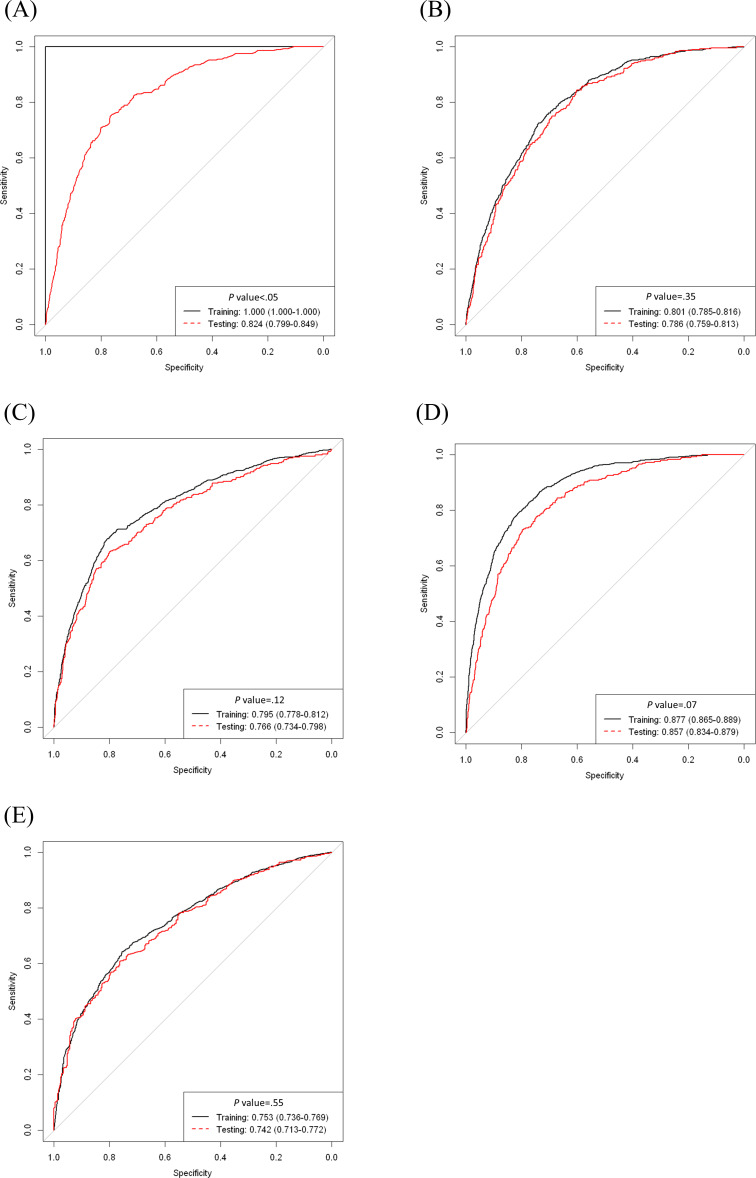
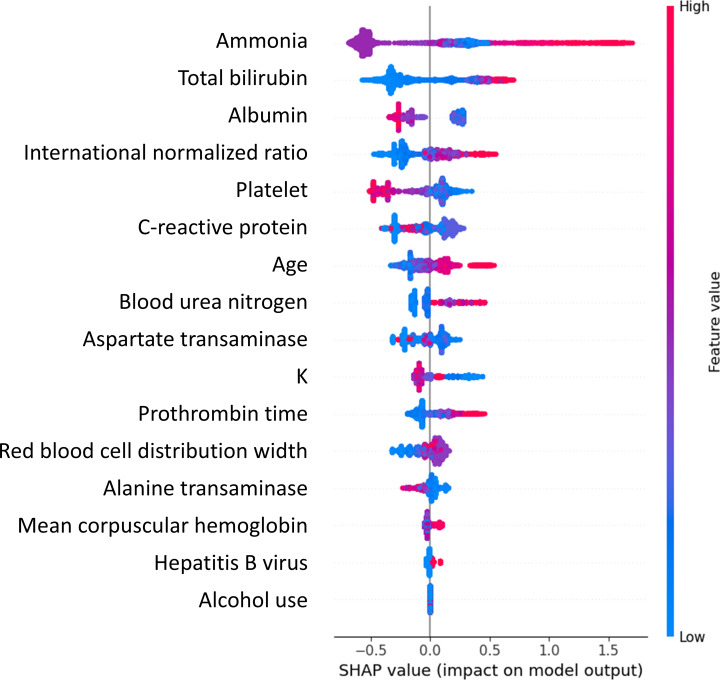
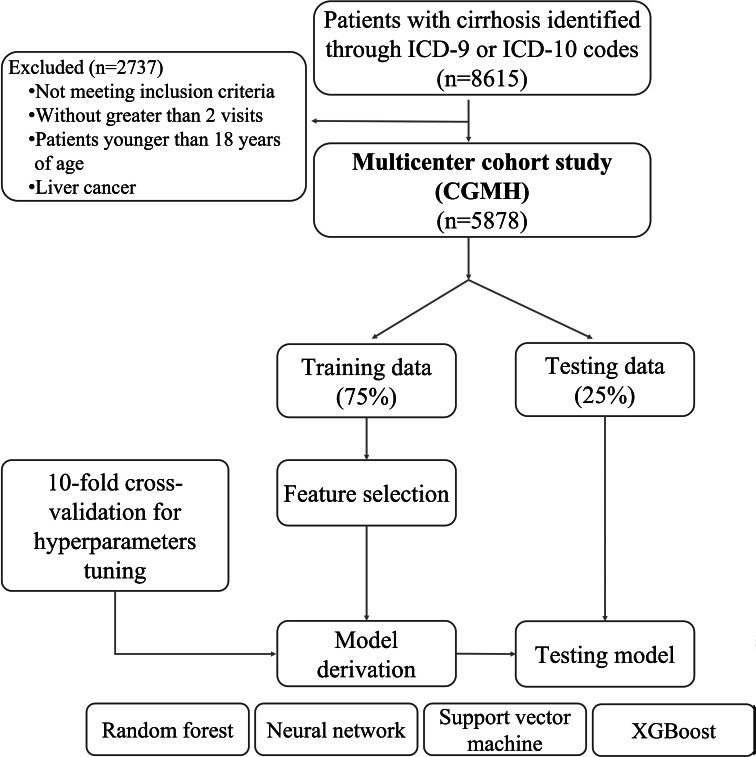
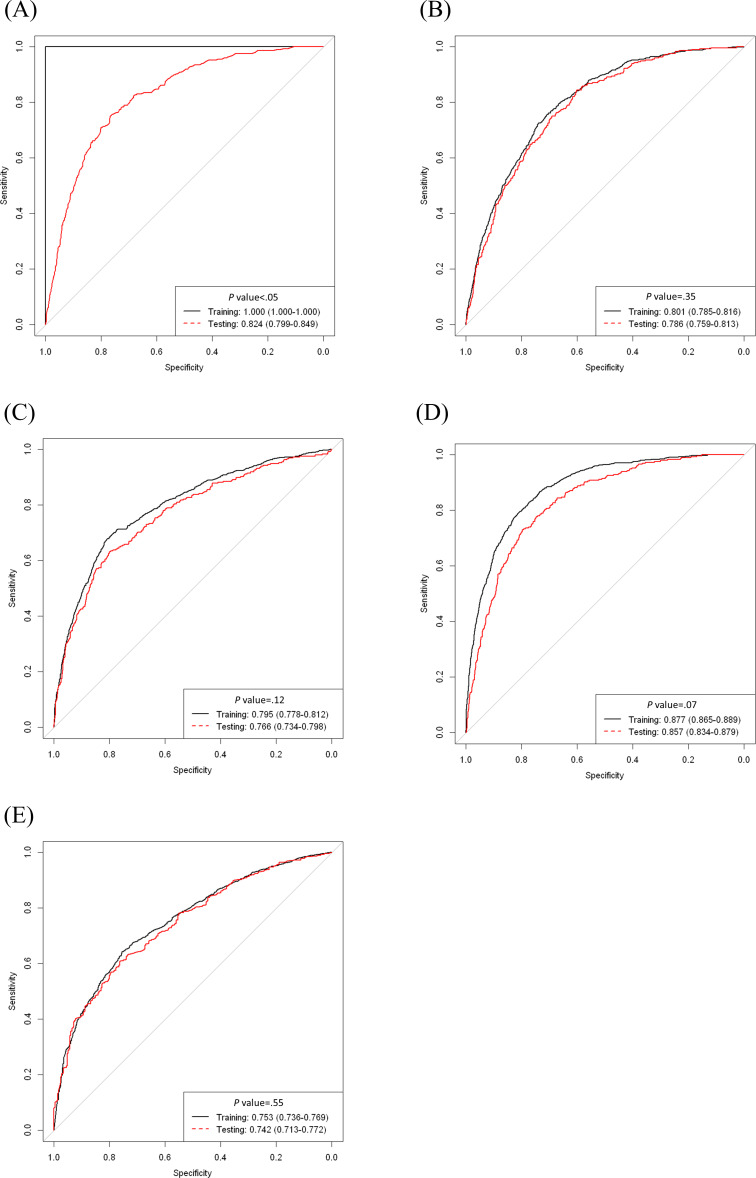
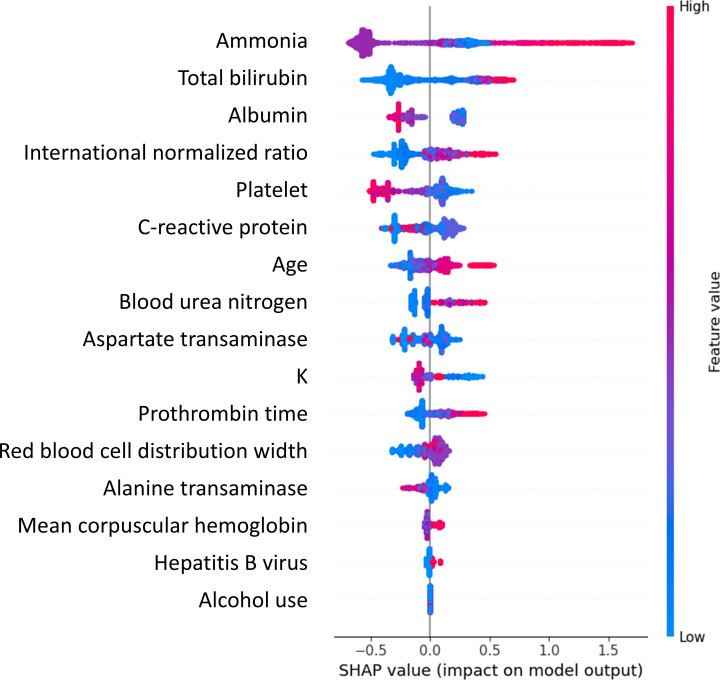
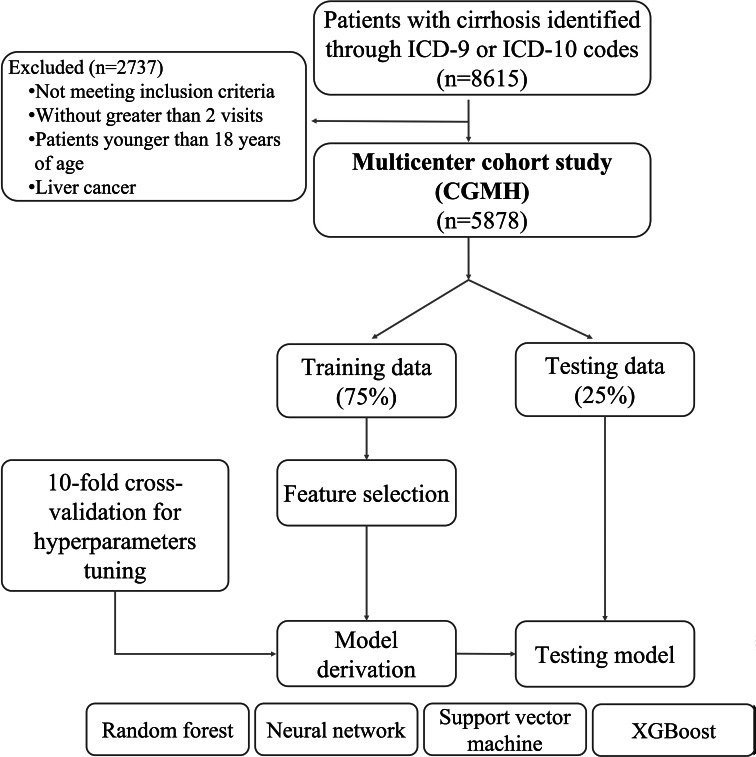
Methods: A multicenter, retrospective cohort study was conducted from January 2010 to December 2017 across all Chang Gung Memorial Hospital branches in northern, middle, and southern Taiwan. We applied several ML models to evaluate HE predictability and compared their performance in the training dataset and testing dataset. Optimal sensitivity and specificity were determined using the Youden index. The best ML model was interpreted by the Shapley Additive Explanations plot.
Results: A total of 5878 patients with cirrhosis were included in the analysis, of whom 1187 (20.2%) subsequently developed HE. Compared to the non-HE group, patients with HE were older (median age 55, IQR 46-65 vs median age 54, IQR 44-66 years; P=.04) and had higher rates of hepatitis B virus infection (351/1187, 30% vs 961/4691, 20.5%; P<.001), alcohol use (540/1187, 45.5% vs 1512/4691, 32.2%; P<.001), sepsis (393/1187, 33.1% vs 792/4691, 16.9%; P<.001), and mortality (425/1187, 35.8% vs 502/4691, 10.7%; P<.001), along with distinct laboratory abnormalities reflecting liver dysfunction. Among the ML algorithms evaluated, the extreme gradient boosting algorithm demonstrated the highest predictive accuracy, achieving an area under the curve (AUC) of 0.86 (95% CI 0.83-0.88) in the testing dataset. This performance was significantly superior to that of the neural network (AUC 0.79, 95% CI 0.76-0.81; P<.001), support vector machine (AUC 0.77, 95% CI 0.73-0.80; P<.001), and the model for end-stage liver disease score (AUC 0.74, 95% CI 0.71-0.77; P<.001). Using a probability threshold of 0.25, the extreme gradient boosting model demonstrated a sensitivity of 72% (95% CI 0.67-0.77), specificity of 80% (95% CI 0.78-0.82), a positive predictive value of 48% (95% CI 43-53), and a negative predictive value of 92% (95% CI 90-94) in the testing set. Comparable performance was observed in the training dataset, with a sensitivity of 80% (95% CI 0.77-0.83), specificity of 81% (95% CI 0.80-0.82), and a negative predictive value of 94% at the same threshold. The most influential predictive variables identified by the model included serum ammonia, aspartate transaminase, alanine transaminase, prothrombin time, and serum potassium.
Conclusions: We developed a novel ML model for predicting HE in patients with noncancer-related cirrhosis. This model provides a practical guide to help physicians and these patients in shared decision-making regarding treatment strategy, with the ultimate goal of improving clinical care and reducing the burden of HE-related morbid complications.
期刊介绍:
JMIR Medical Informatics (JMI, ISSN 2291-9694) is a top-rated, tier A journal which focuses on clinical informatics, big data in health and health care, decision support for health professionals, electronic health records, ehealth infrastructures and implementation. It has a focus on applied, translational research, with a broad readership including clinicians, CIOs, engineers, industry and health informatics professionals.
Published by JMIR Publications, publisher of the Journal of Medical Internet Research (JMIR), the leading eHealth/mHealth journal (Impact Factor 2016: 5.175), JMIR Med Inform has a slightly different scope (emphasizing more on applications for clinicians and health professionals rather than consumers/citizens, which is the focus of JMIR), publishes even faster, and also allows papers which are more technical or more formative than what would be published in the Journal of Medical Internet Research.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


