Zhiqiang Shi, Pengfei Qiu, Yongsheng Wang, Hong Liu
{"title":"Minimally invasive biopsy technique predicting breast pathological complete response after neoadjuvant therapy for breast cancer.","authors":"Zhiqiang Shi, Pengfei Qiu, Yongsheng Wang, Hong Liu","doi":"10.21037/gs-2025-103","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Neoadjuvant therapy (NAT) is widely used in the treatment of breast cancer, and the pathological complete response (pCR) rate is increasing. However, currently, the prediction of pCR still lacks accuracy. This study aimed to investigate the accuracy of minimally invasive biopsy techniques in predicting breast pCR (bpCR) after NAT in breast cancer.</p><p><strong>Methods: </strong>From October 2022 to October 2024, a prospective single-arm study was conducted on 132 patients with primary breast cancer who achieved breast radiologic complete response (brCR) or breast radiologic partial response (brPR) after NAT at the Breast Center of Shandong Cancer Hospital. Before NAT, a marker clip was placed at the center of the tumor bed. After NAT, in patients with no residual lesions suggested by ultrasound, iodine-125 was placed under the guidance of mammography, followed by routine breast surgery (breast-conserving surgery or mastectomy). Postoperatively, multiple-site core needle biopsy (CNB) under ultrasound guidance was performed on the surgical specimen. The pathological results of CNB specimens were compared with those of surgical specimens to assess the accuracy of CNB in predicting bpCR (ypT0) after NAT.</p><p><strong>Results: </strong>A total of 52 patients (39.4%) achieved bpCR after NAT. Univariate analysis showed that tumor molecular subtypes, brCR after NAT, and axillary pathological complete response (apCR) were significantly associated with bpCR (P=0.02, 0.02, and P<0.001, respectively). Ultrasound-guided multiple-site CNB had an accuracy, negative predictive value (NPV), and false-negative rate (FNR) of 90.9%, 81.0%, and 14.8%, respectively, in predicting bpCR after NAT, which were superior to those of ultrasound, mammography, and magnetic resonance imaging. The combination of imaging examinations and ultrasound-guided multiple-site CNB significantly reduced the FNR compared with CNB alone (7.4% <i>vs.</i> 14.8%; P<0.001). No false-negative results were found in 45 cases using large-bore CNB needles (12G).</p><p><strong>Conclusions: </strong>The combination of imaging examinations and ultrasound-guided multiple-site CNB has the potential to accurately predict bpCR after NAT, making it possible to selectively avoid breast surgery in breast cancer patients after NAT.</p>","PeriodicalId":12760,"journal":{"name":"Gland surgery","volume":"14 7","pages":"1263-1271"},"PeriodicalIF":1.6000,"publicationDate":"2025-07-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12322751/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gland surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/gs-2025-103","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/28 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Neoadjuvant therapy (NAT) is widely used in the treatment of breast cancer, and the pathological complete response (pCR) rate is increasing. However, currently, the prediction of pCR still lacks accuracy. This study aimed to investigate the accuracy of minimally invasive biopsy techniques in predicting breast pCR (bpCR) after NAT in breast cancer.
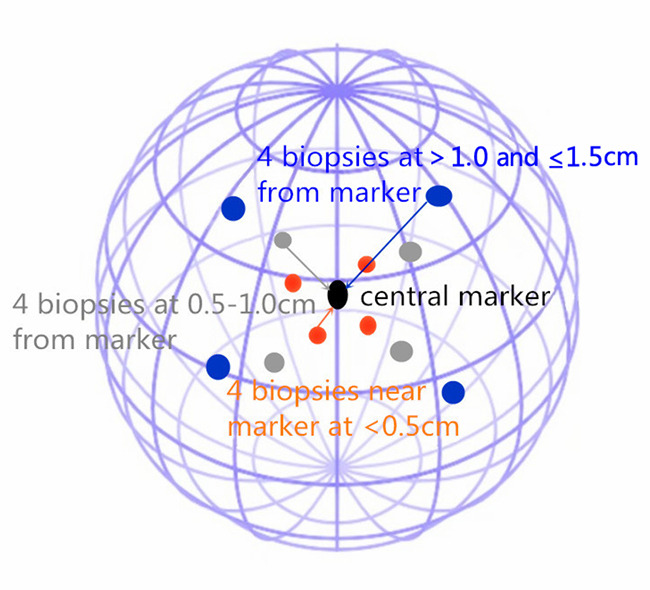
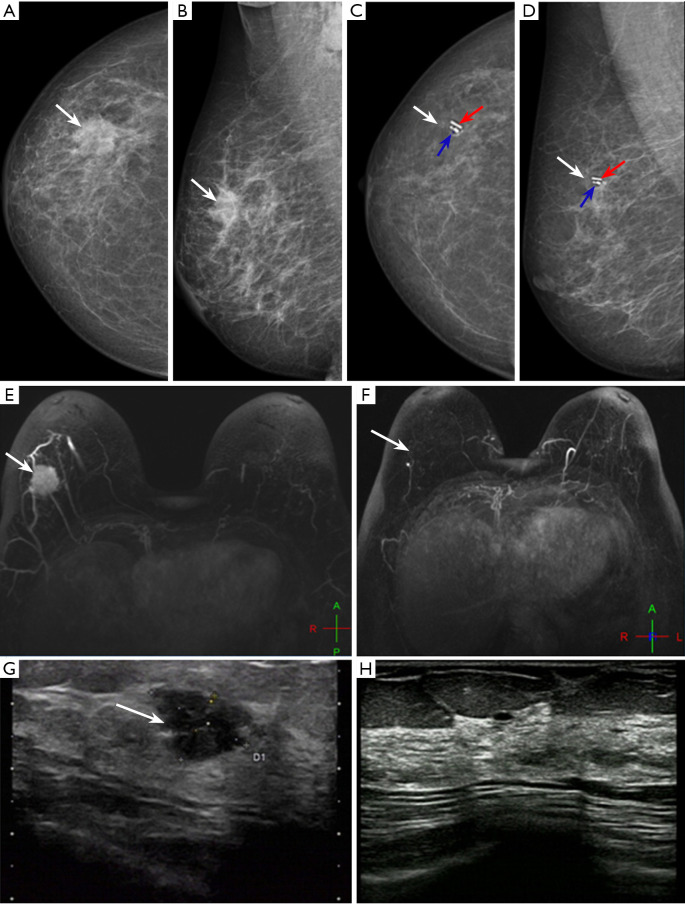
Methods: From October 2022 to October 2024, a prospective single-arm study was conducted on 132 patients with primary breast cancer who achieved breast radiologic complete response (brCR) or breast radiologic partial response (brPR) after NAT at the Breast Center of Shandong Cancer Hospital. Before NAT, a marker clip was placed at the center of the tumor bed. After NAT, in patients with no residual lesions suggested by ultrasound, iodine-125 was placed under the guidance of mammography, followed by routine breast surgery (breast-conserving surgery or mastectomy). Postoperatively, multiple-site core needle biopsy (CNB) under ultrasound guidance was performed on the surgical specimen. The pathological results of CNB specimens were compared with those of surgical specimens to assess the accuracy of CNB in predicting bpCR (ypT0) after NAT.
Results: A total of 52 patients (39.4%) achieved bpCR after NAT. Univariate analysis showed that tumor molecular subtypes, brCR after NAT, and axillary pathological complete response (apCR) were significantly associated with bpCR (P=0.02, 0.02, and P<0.001, respectively). Ultrasound-guided multiple-site CNB had an accuracy, negative predictive value (NPV), and false-negative rate (FNR) of 90.9%, 81.0%, and 14.8%, respectively, in predicting bpCR after NAT, which were superior to those of ultrasound, mammography, and magnetic resonance imaging. The combination of imaging examinations and ultrasound-guided multiple-site CNB significantly reduced the FNR compared with CNB alone (7.4% vs. 14.8%; P<0.001). No false-negative results were found in 45 cases using large-bore CNB needles (12G).
Conclusions: The combination of imaging examinations and ultrasound-guided multiple-site CNB has the potential to accurately predict bpCR after NAT, making it possible to selectively avoid breast surgery in breast cancer patients after NAT.
期刊介绍:
Gland Surgery (Gland Surg; GS, Print ISSN 2227-684X; Online ISSN 2227-8575) being indexed by PubMed/PubMed Central, is an open access, peer-review journal launched at May of 2012, published bio-monthly since February 2015.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


