{"title":"Dorsoradial vs. circular cast for distal radius fractures: a retrospective comparative cohort study.","authors":"Oğuzhan Gökalp, Gökhan Ilyas","doi":"10.14744/tjtes.2025.80448","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Non-articular dorsally angulated distal radius fractures (DRFs) are often managed conservatively, yet the optimal cast design remains debated. Dorsoradial (DR) casting leaves the ulnar border open, potentially better accommodating swelling and reducing early cast-related interventions.</p><p><strong>Methods: </strong>A single-center retrospective cohort study included adults with AO-23-A2/A3 DRFs treated between May 2019 and May 2023. Patients received either a DR cast (n=88) or a conventional circular cast (CC) (n=122) for a standard five-week immobilization. Primary outcomes included functional (Patient-Rated Wrist Evaluation, PRWE) and clinical (Gartland-Werley, GW) scores, along with radiographic alignment (volar tilt, radial inclination, radial height) at a median follow-up of 118.5 weeks. Secondary outcomes were early cast revisions (release or reinforcement) and complications. Statistical tests included Mann-Whitney U, χ²/Fisher, with Bonferroni-adjusted α=0.017.</p><p><strong>Results: </strong>Baseline characteristics were similar across groups: mean age 60±11 years, 87% female, comparable AO subtype distribution, and osteoporosis status. Early revision: DR 22.7% vs. CC 36.1% (absolute risk reduction 13% points; odds ratio: 0.51, p=0.038), primarily due to fewer cast releases for swelling/pain (12.5% vs. 32.8%, p=0.001). Function: PRWE scores were 34±18 (DR) vs. 36±18 (CC), p=0.435; GW scores were good-excellent in 79.5% vs. 77.8%, p=0.508. Radiographic outcomes: final volar tilt and radial height were similar (both p>0.08). DR casts better preserved radial inclination (median change 0°, p=0.057) compared to CC casts, which lost 1.3° (-6%, p<0.001); however, the net 1.2° intergroup difference is below the 5° minimal clinically important difference (MCID) and is clinically negligible. No cases of compartment syndrome or acute carpal tunnel occurred.</p><p><strong>Conclusion: </strong>Dorsoradial casting delivers functional and radiographic outcomes equivalent to circular casting while reducing early revision rates by one-fifth. By lowering unplanned cast adjustments and follow-up visits, the DR technique represents a pragmatic alternative for centers with limited monitoring capacity treating dorsally angulated extra-articular DRFs.</p>","PeriodicalId":94263,"journal":{"name":"Ulusal travma ve acil cerrahi dergisi = Turkish journal of trauma & emergency surgery : TJTES","volume":"31 8","pages":"789-797"},"PeriodicalIF":1.0000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12363139/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ulusal travma ve acil cerrahi dergisi = Turkish journal of trauma & emergency surgery : TJTES","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14744/tjtes.2025.80448","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Non-articular dorsally angulated distal radius fractures (DRFs) are often managed conservatively, yet the optimal cast design remains debated. Dorsoradial (DR) casting leaves the ulnar border open, potentially better accommodating swelling and reducing early cast-related interventions.
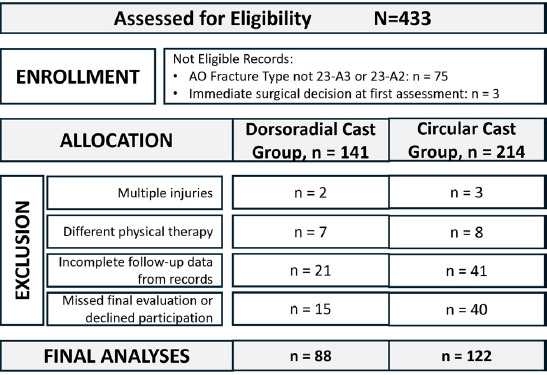
Methods: A single-center retrospective cohort study included adults with AO-23-A2/A3 DRFs treated between May 2019 and May 2023. Patients received either a DR cast (n=88) or a conventional circular cast (CC) (n=122) for a standard five-week immobilization. Primary outcomes included functional (Patient-Rated Wrist Evaluation, PRWE) and clinical (Gartland-Werley, GW) scores, along with radiographic alignment (volar tilt, radial inclination, radial height) at a median follow-up of 118.5 weeks. Secondary outcomes were early cast revisions (release or reinforcement) and complications. Statistical tests included Mann-Whitney U, χ²/Fisher, with Bonferroni-adjusted α=0.017.
Results: Baseline characteristics were similar across groups: mean age 60±11 years, 87% female, comparable AO subtype distribution, and osteoporosis status. Early revision: DR 22.7% vs. CC 36.1% (absolute risk reduction 13% points; odds ratio: 0.51, p=0.038), primarily due to fewer cast releases for swelling/pain (12.5% vs. 32.8%, p=0.001). Function: PRWE scores were 34±18 (DR) vs. 36±18 (CC), p=0.435; GW scores were good-excellent in 79.5% vs. 77.8%, p=0.508. Radiographic outcomes: final volar tilt and radial height were similar (both p>0.08). DR casts better preserved radial inclination (median change 0°, p=0.057) compared to CC casts, which lost 1.3° (-6%, p<0.001); however, the net 1.2° intergroup difference is below the 5° minimal clinically important difference (MCID) and is clinically negligible. No cases of compartment syndrome or acute carpal tunnel occurred.
Conclusion: Dorsoradial casting delivers functional and radiographic outcomes equivalent to circular casting while reducing early revision rates by one-fifth. By lowering unplanned cast adjustments and follow-up visits, the DR technique represents a pragmatic alternative for centers with limited monitoring capacity treating dorsally angulated extra-articular DRFs.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


